Downloaded 393 times
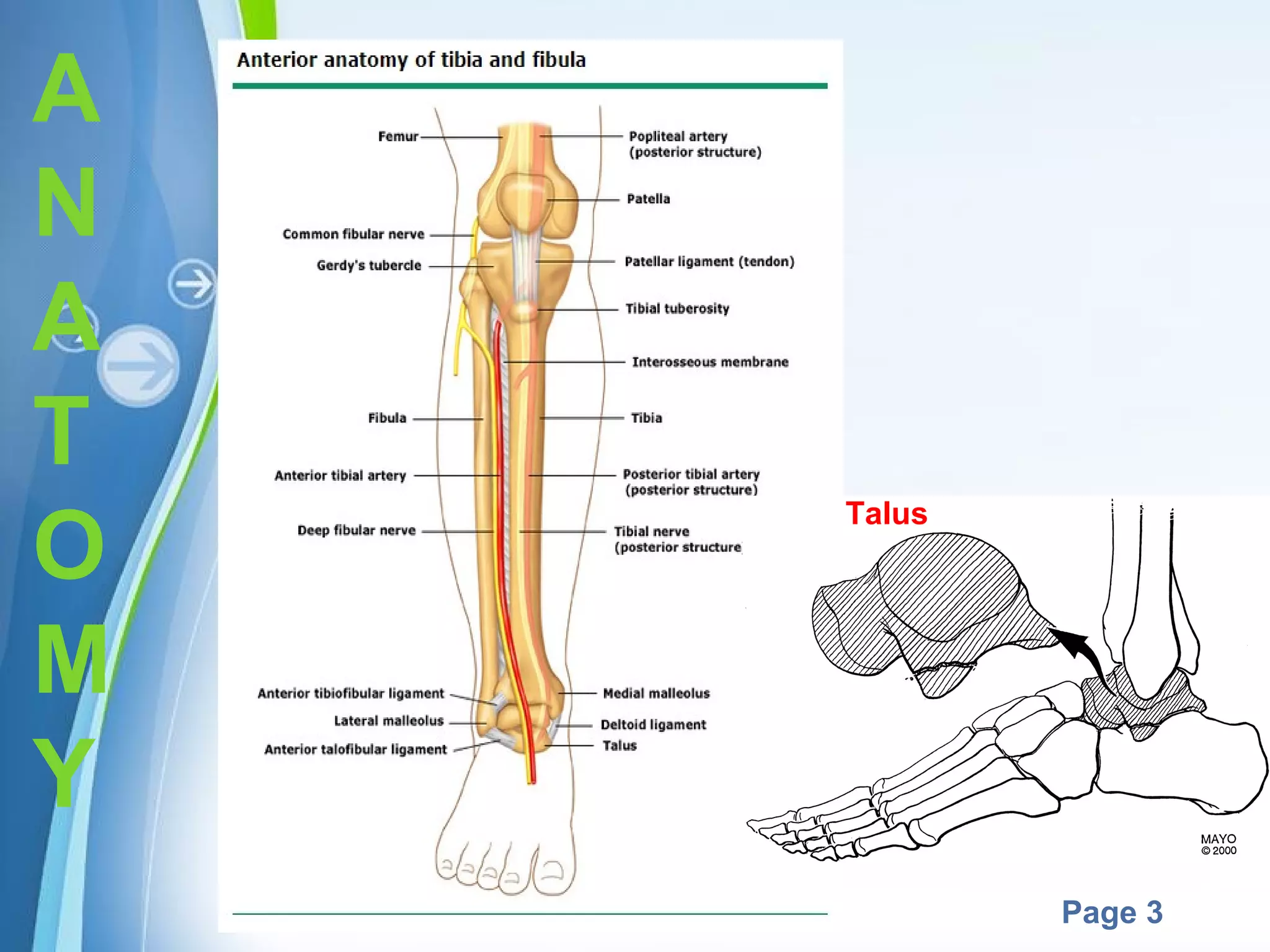
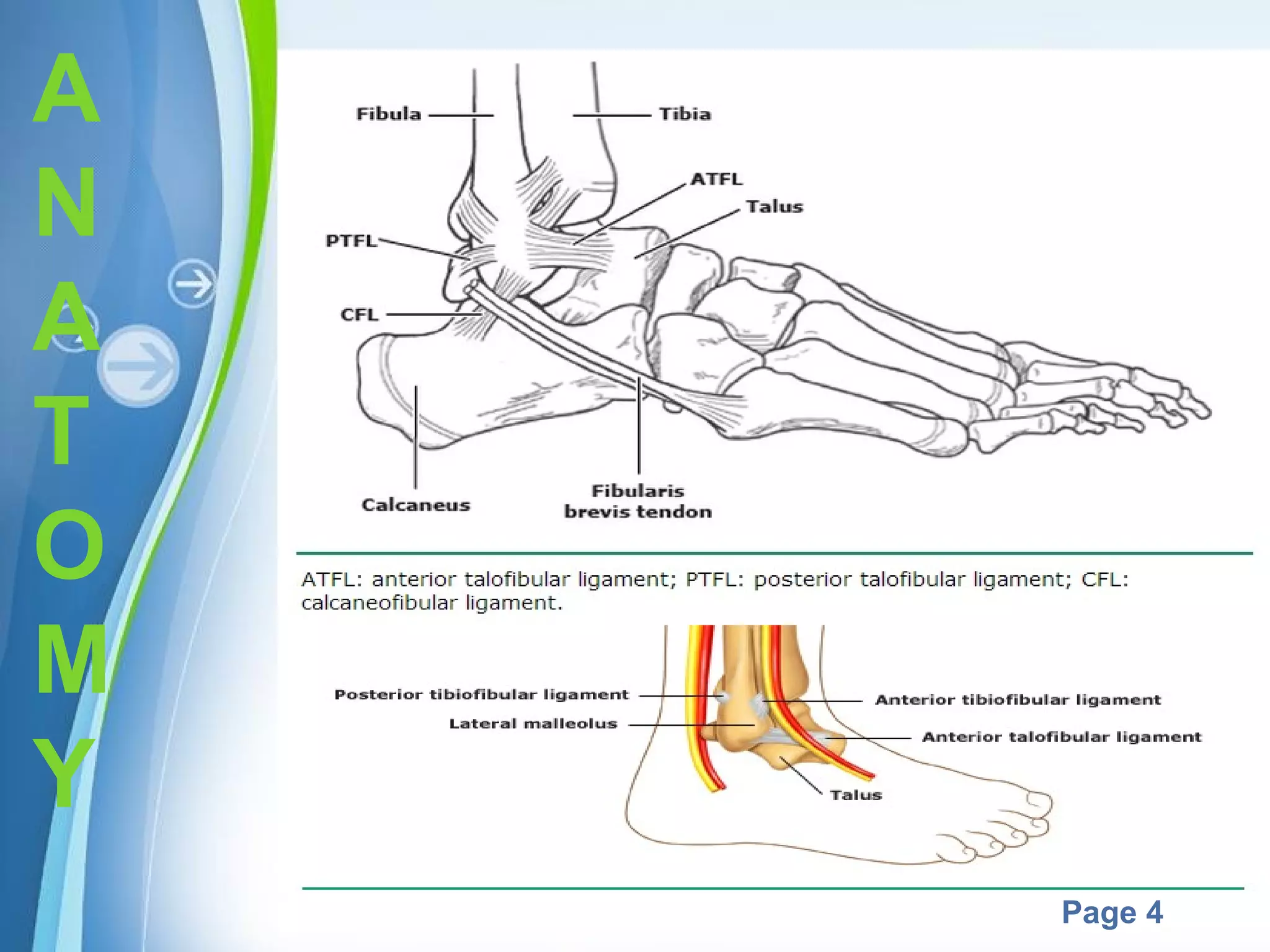
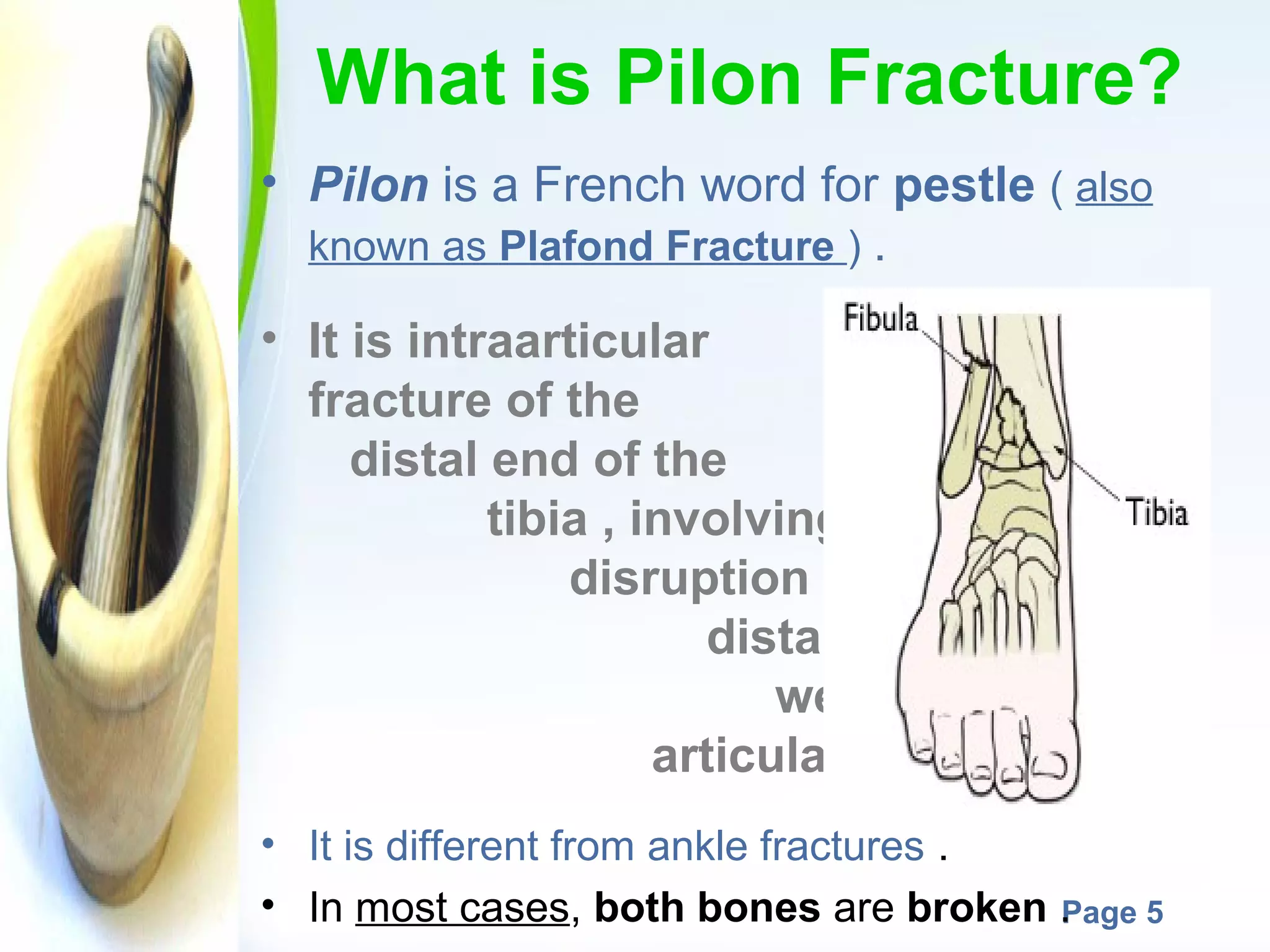

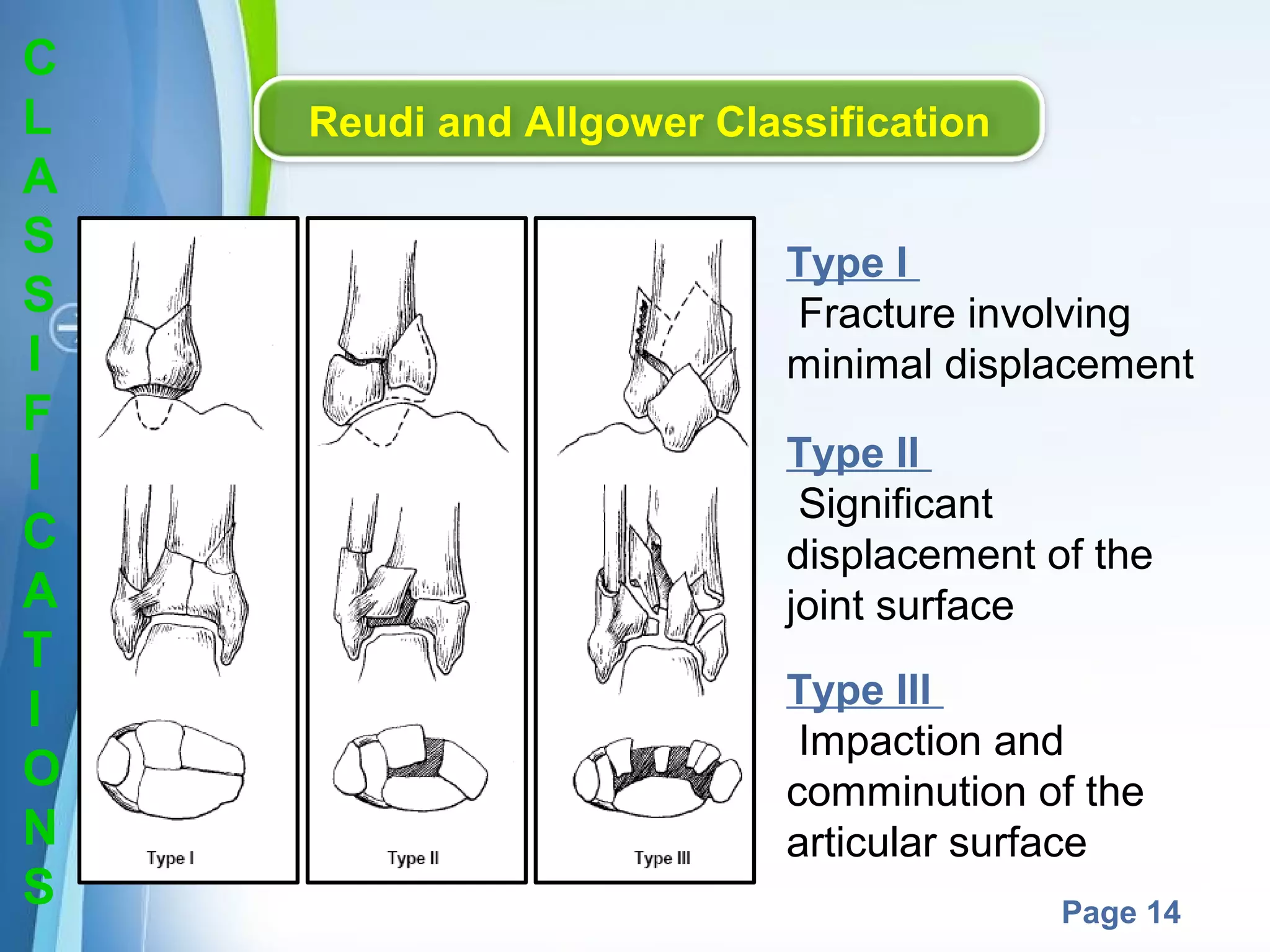
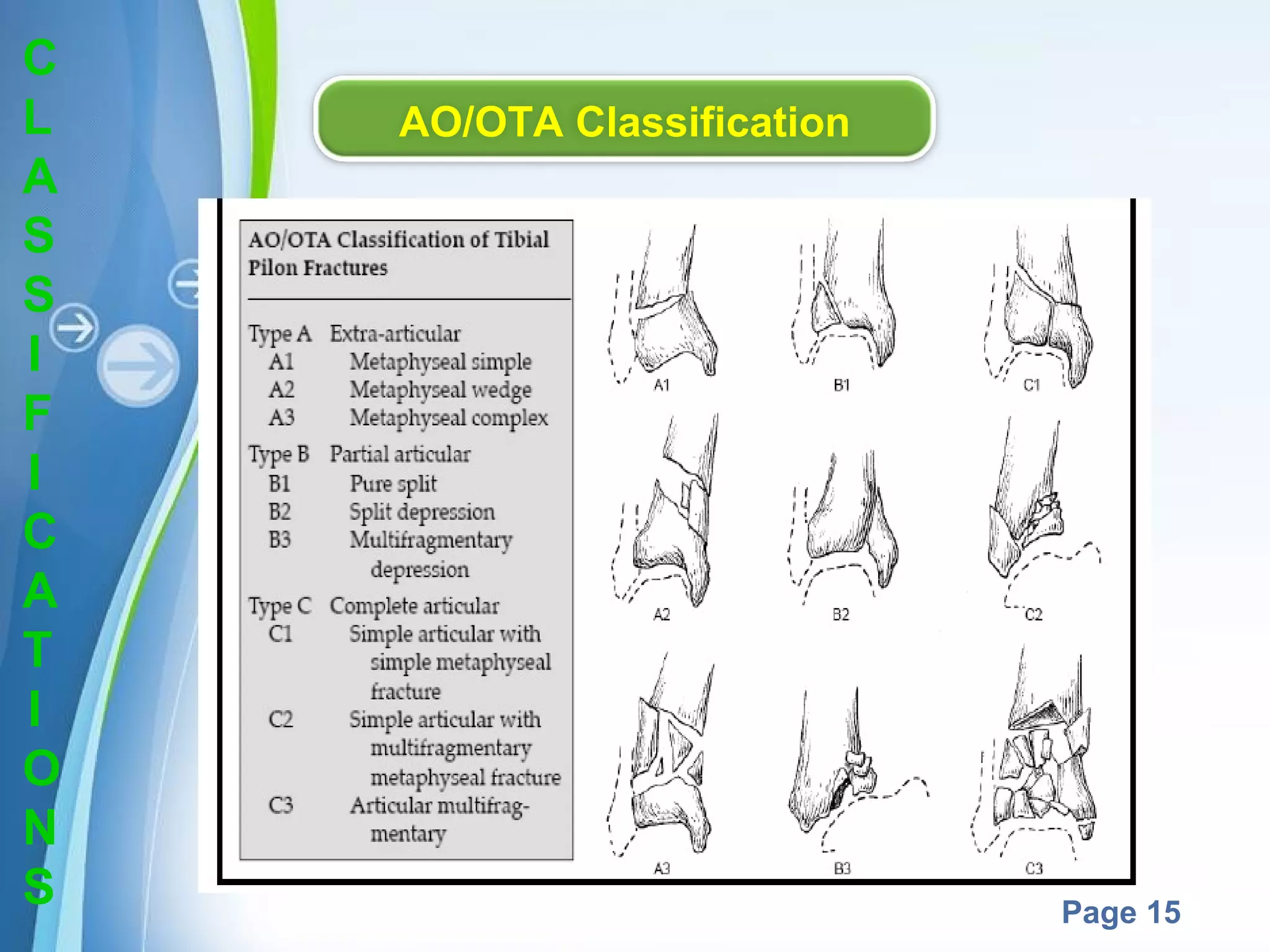




This document is a presentation on Pilon fractures, which are intra-articular fractures of the distal tibia. The presentation covers the anatomy, definition, epidemiology, mechanisms of injury, evaluation including clinical presentation, physical exam and imaging, classifications systems, associated injuries, treatment goals and options, complications, and surgical techniques for treatment. The overall objectives are to provide an overview of Pilon fractures and discuss evaluation, classification, treatment and complications.































































































