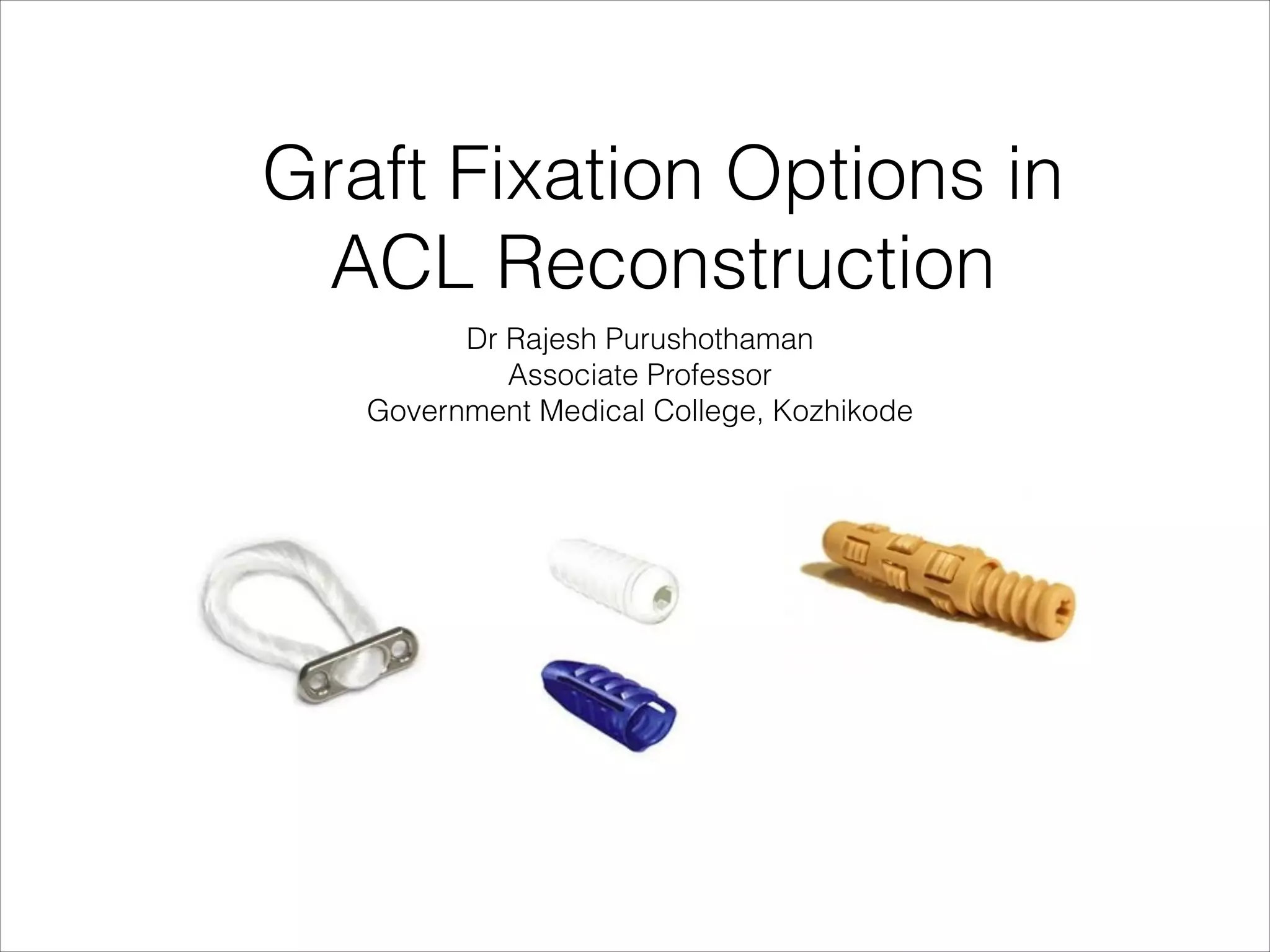







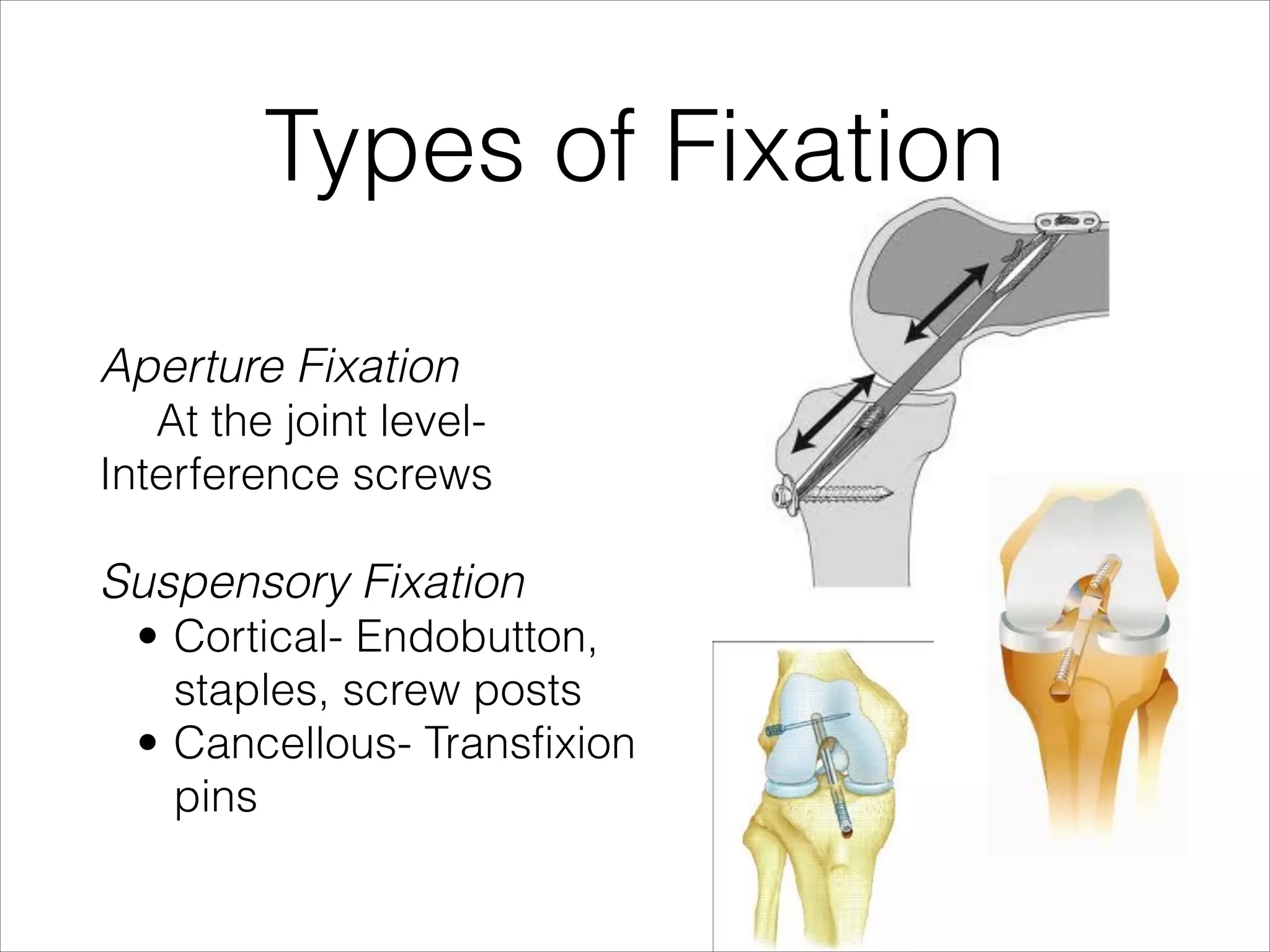






















The document discusses graft fixation options in ACL reconstruction. It notes that fixation is the weakest link in the early postoperative period and that tibial fixation carries a greater risk of failure. Interference screws provide the gold standard for fixation but tunnel widening remains a concern. The ideal fixation is strong, stiff, and secure to avoid graft slippage and interference with healing while allowing revision. Aperture fixation and hybrid techniques may improve outcomes over suspensory fixation alone. Rehabilitation must also account for the biomechanical strengths and weaknesses of the fixation method used.












































































