Downloaded 1,645 times



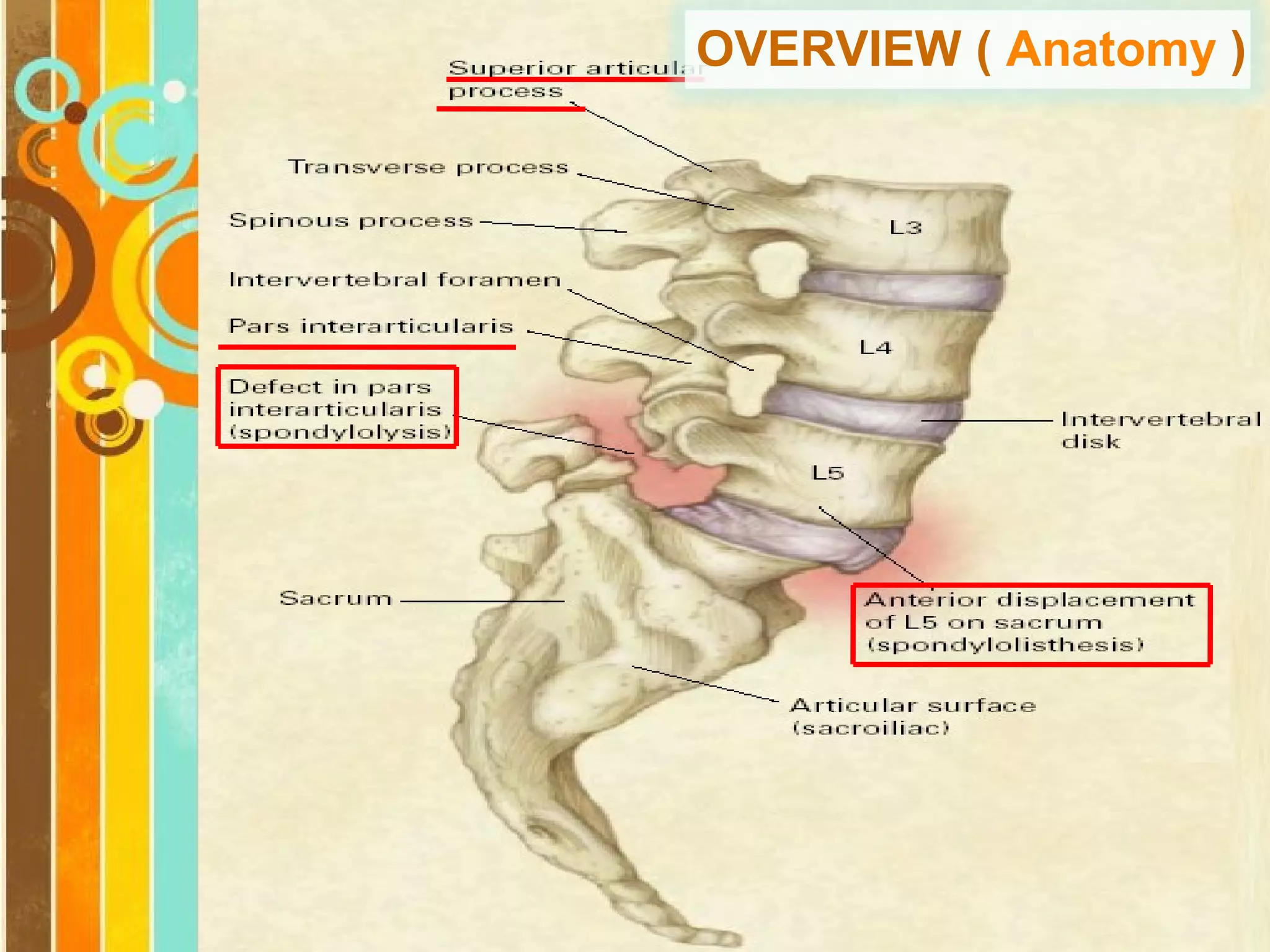

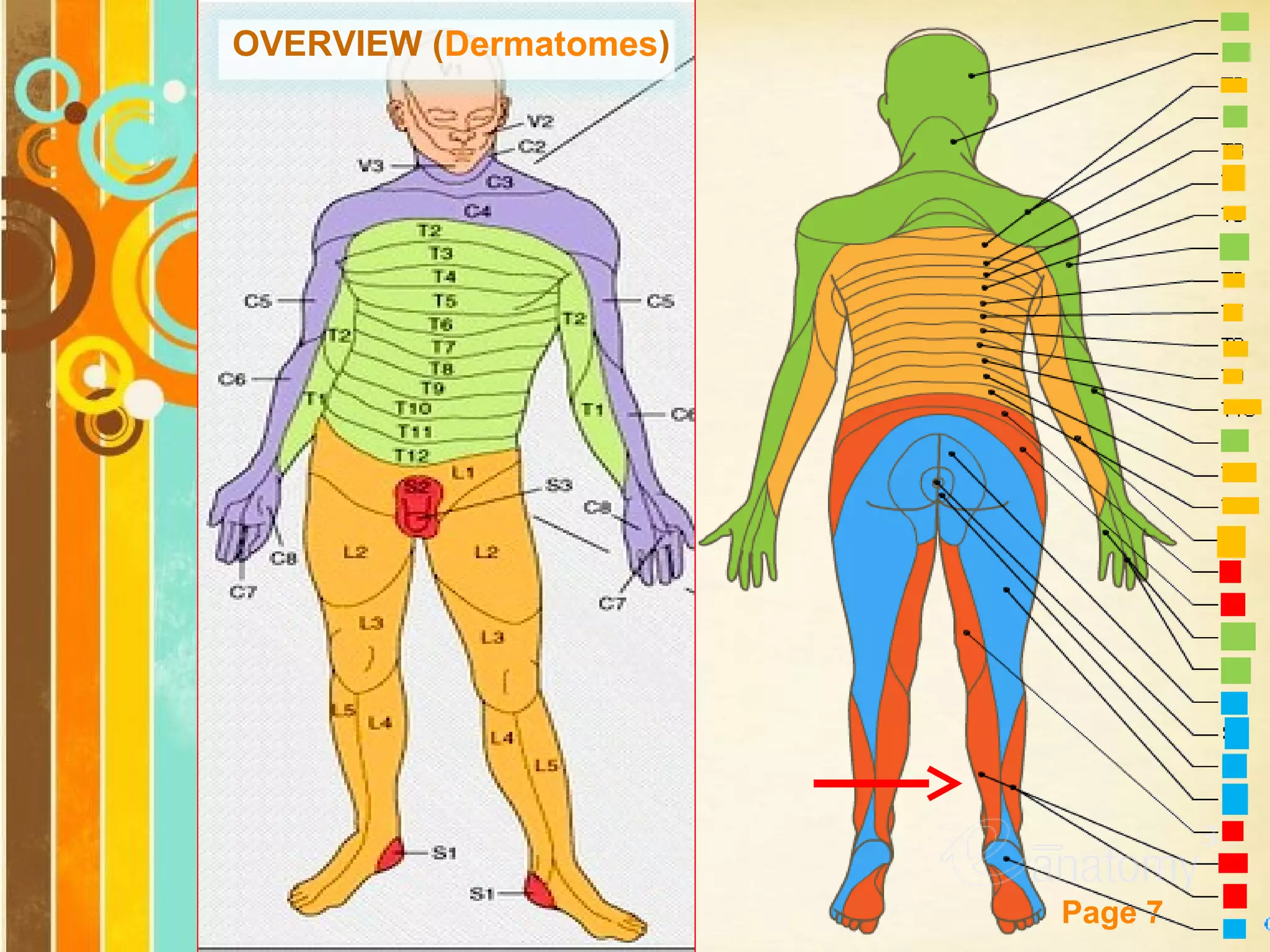



















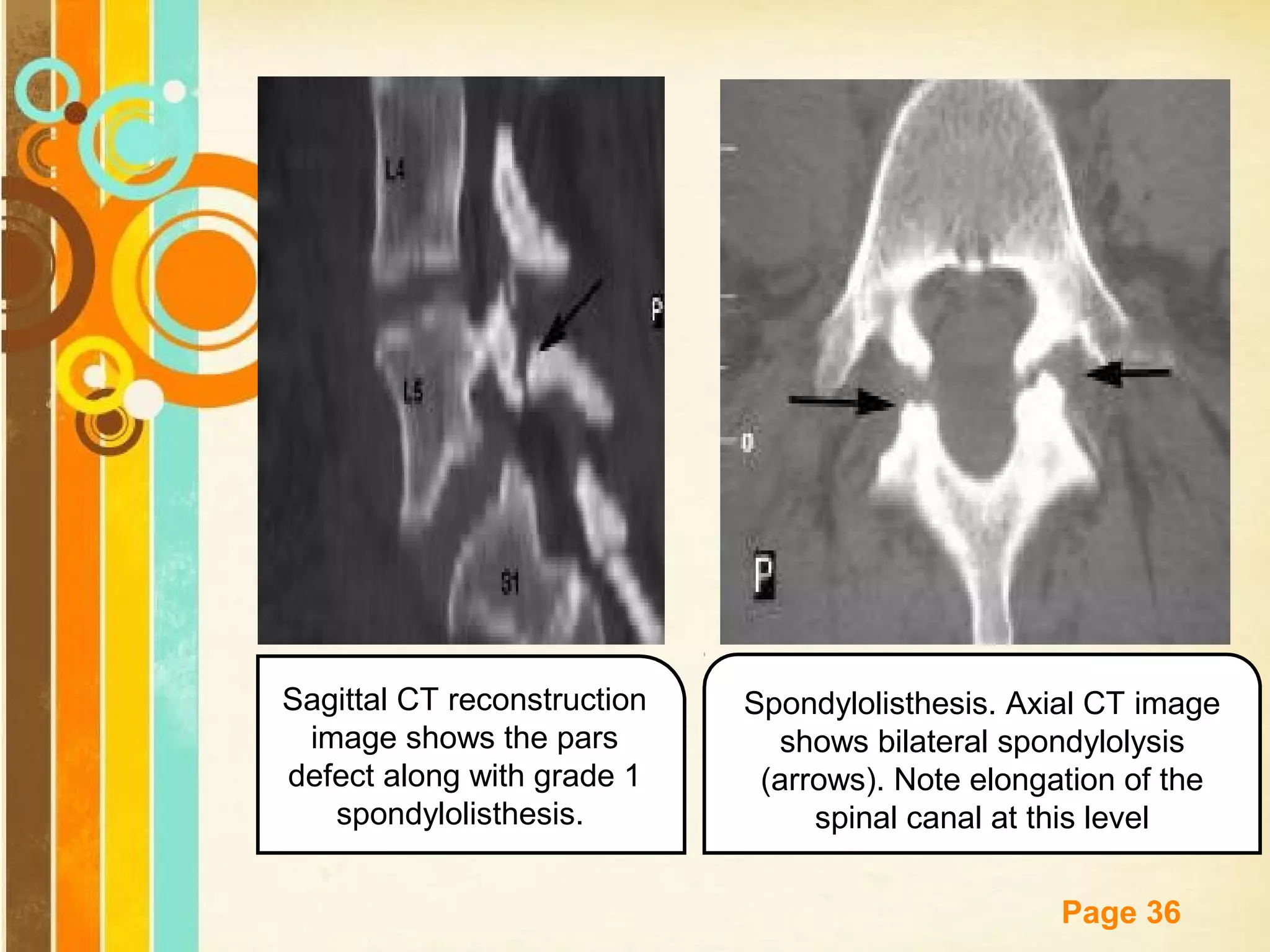





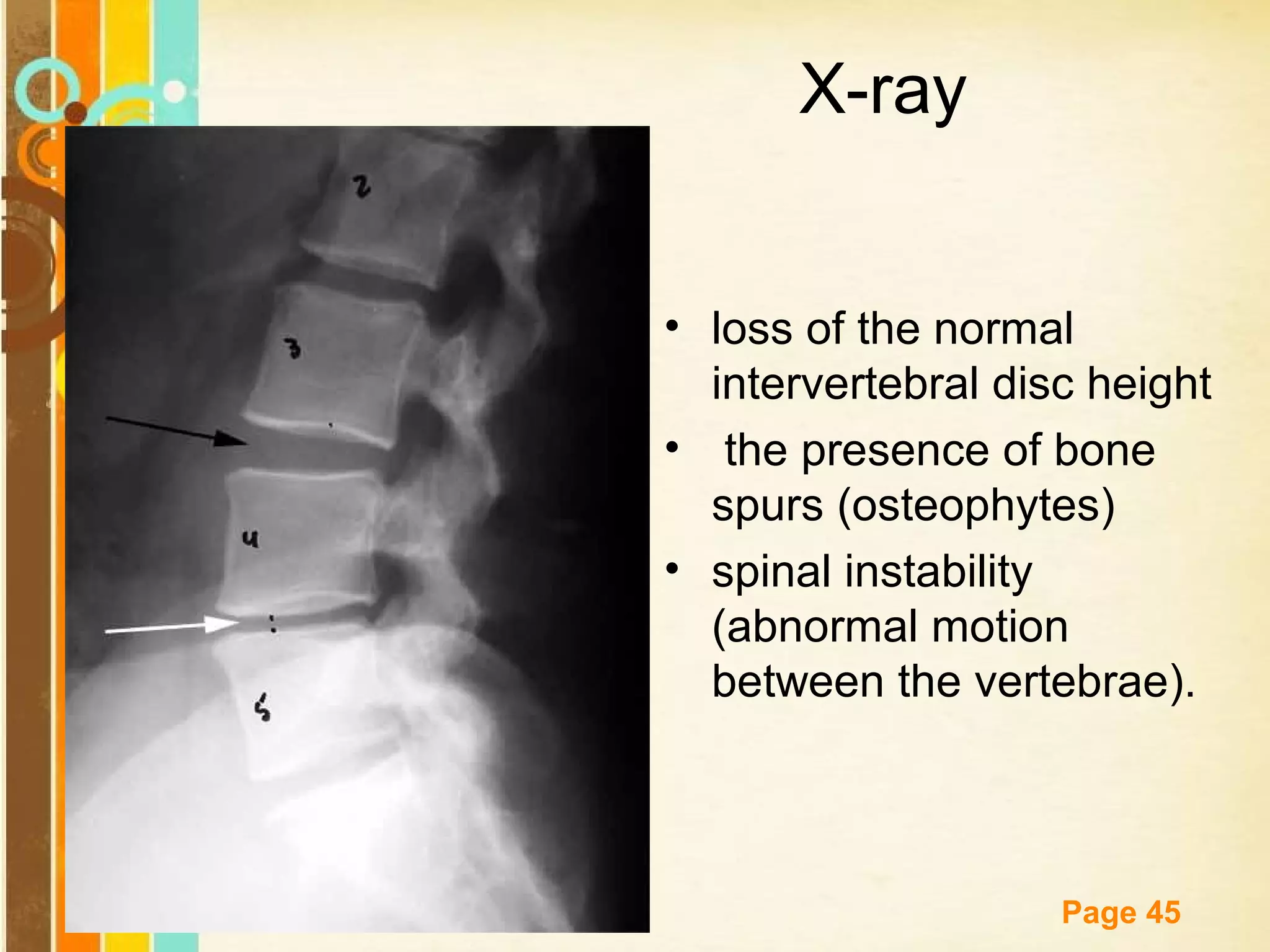


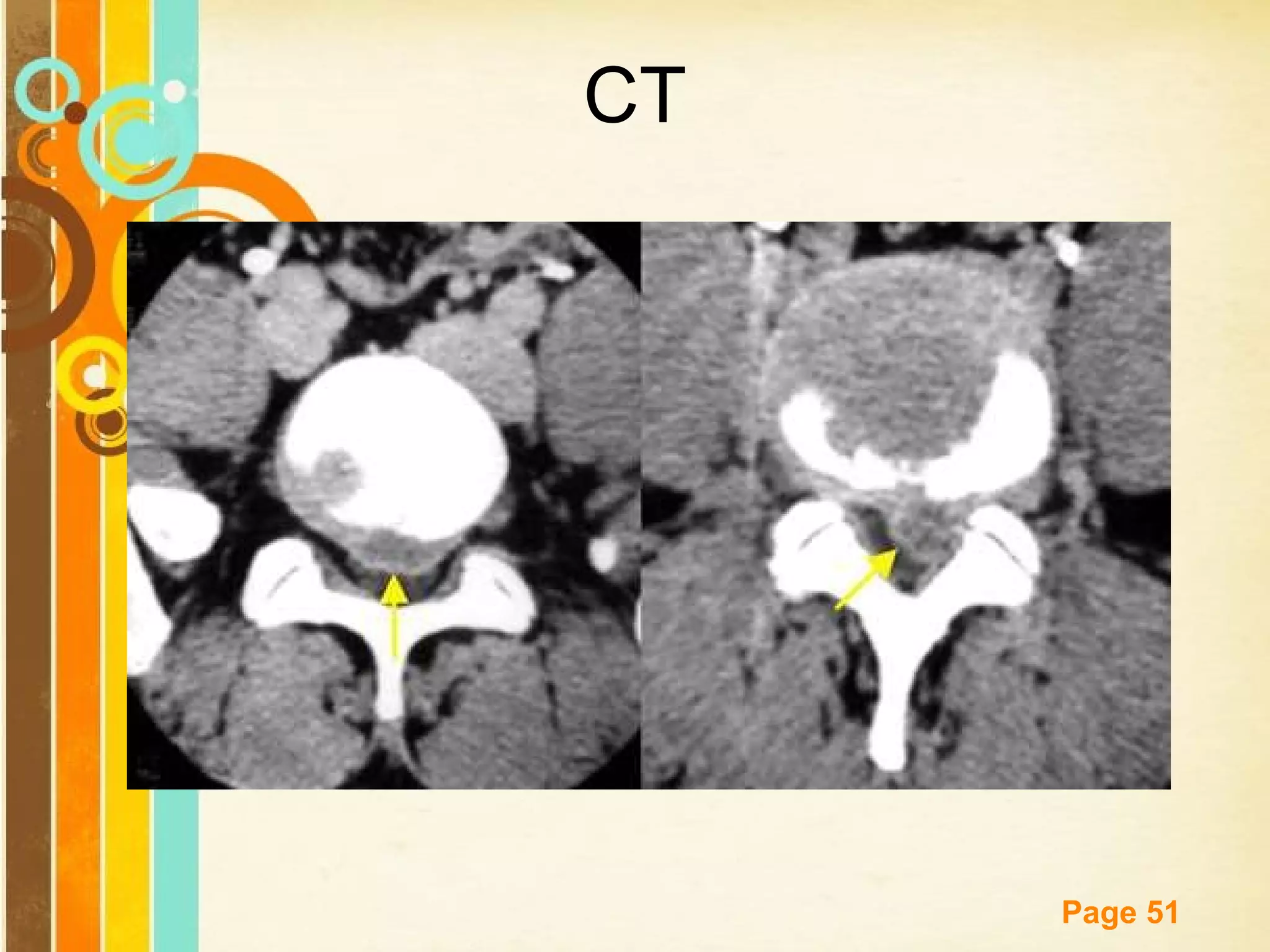












1) Spondylolisthesis is the forward slippage of one vertebra over another, usually occurring at L5-S1. It is commonly caused by defects in the pars interarticularis (spondylolysis), which allows stress fractures and slippage. 2) Common symptoms include low back pain exacerbated by movement and radiating pain or numbness in the legs. Physical exam may reveal tenderness over the slipped vertebrae, muscle spasms, and limited flexion. 3) Diagnosis is made through imaging like x-rays, CT, or MRI. X-rays can grade the percentage of slippage. CT and MRI better visualize defects and any impinge











































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)