Downloaded 95 times
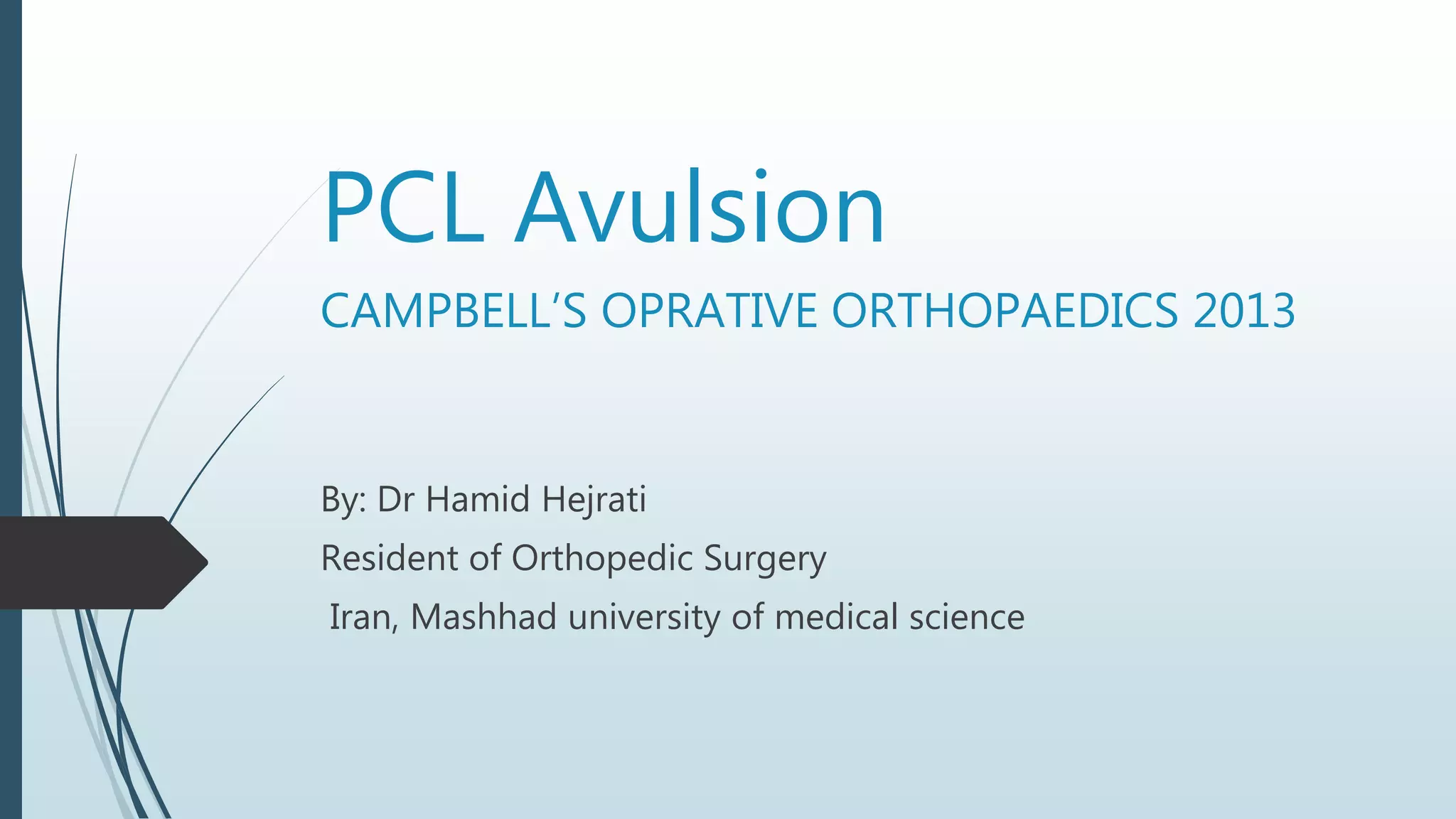







1) PCL avulsion injuries involve the tearing of the PCL from the tibia, often with a bone fragment. Arthroscopic examination is required before surgical repair through a posterior approach to check for other knee injuries. 2) Surgical repair of a PCL avulsion involves exposing the tibial attachment through a medial or posterior approach. The bone fragment is reattached using screws or sutures passed through drill holes. The posterior capsule is also repaired with sutures. 3) Postoperative care following PCL avulsion repair involves the use of a hinged knee brace, touch-down weight bearing, and a physical therapy regimen focusing on range of motion and strengthening exercises.













































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








