Downloaded 13 times
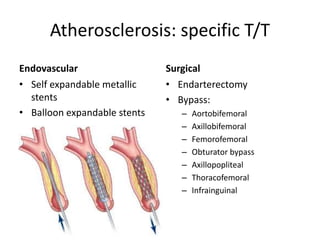

This document discusses ischaemia of the lower limbs, including definitions, causes, clinical features, investigations and management. Some key points: - Peripheral vascular disease refers to obstruction or deterioration of arteries other than those supplying the heart or brain. - Causes of acute limb ischaemia include embolism (often from the heart) and thrombosis (due to atherosclerosis, aneurysm, etc.). - Clinical features depend on location and duration of ischaemia, and can include pain, pallor, pulselessness, paralysis. Beyond 6 hours ischemia is usually irreversible. - Investigations include blood tests, imaging like Doppler ultrasound and angiography. Management involves treating the cause, and surgical

















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



