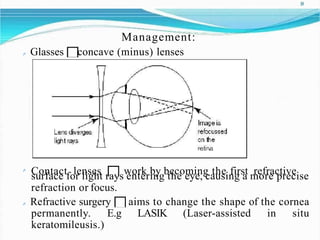
Types of refractive errors include myopia, hyperopia, astigmatism, presbyopia, and anisometropia. Myopia occurs when light focuses in front of the retina, causing near-sightedness. Hyperopia is the opposite where light focuses behind the retina, causing far-sightedness. Astigmatism results from an irregularly shaped cornea or lens that causes blurred vision. Presbyopia is the natural aging of the lens that makes close vision difficult. Anisometropia is a difference in refractive error between the two eyes. Management options for refractive errors include glasses, contact lenses, refractive surgery, and orthokeratology.