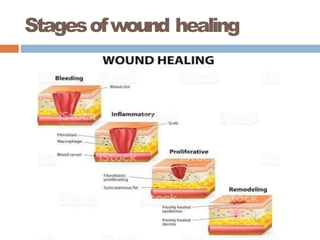
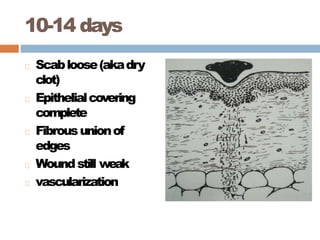
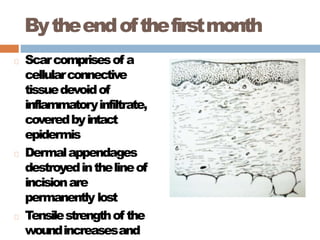
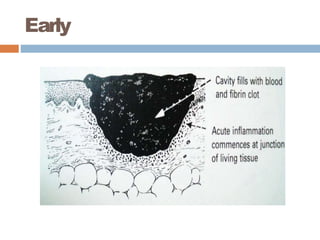
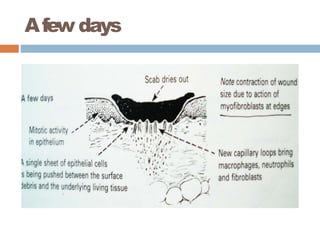
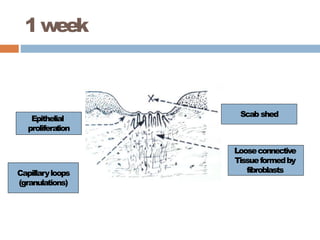
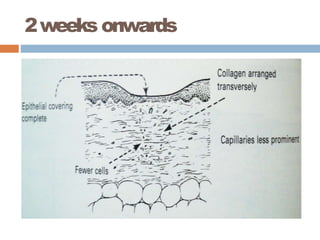
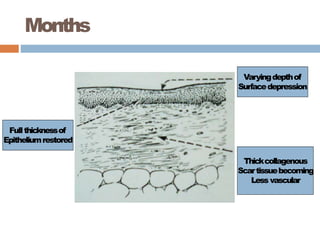
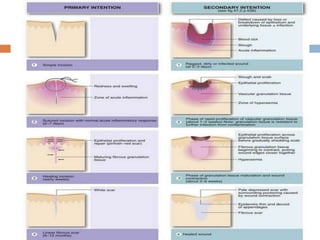
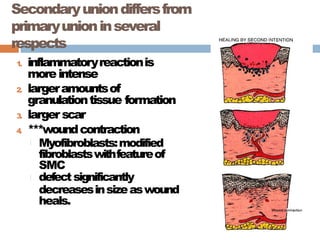
Wound healing occurs in 3 phases: inflammatory, proliferative, and remodeling. The inflammatory phase involves hemostasis, recruitment of inflammatory cells, and initiation of tissue regeneration. During the proliferative phase, granulation tissue forms through angiogenesis, fibroblast proliferation, and epithelialization. In the remodeling phase, collagen deposition increases wound strength over months. Wound healing can occur through primary intention in clean wounds or secondary intention in wounds with tissue loss, involving more granulation tissue formation and contraction. Systemic and local factors can influence healing.