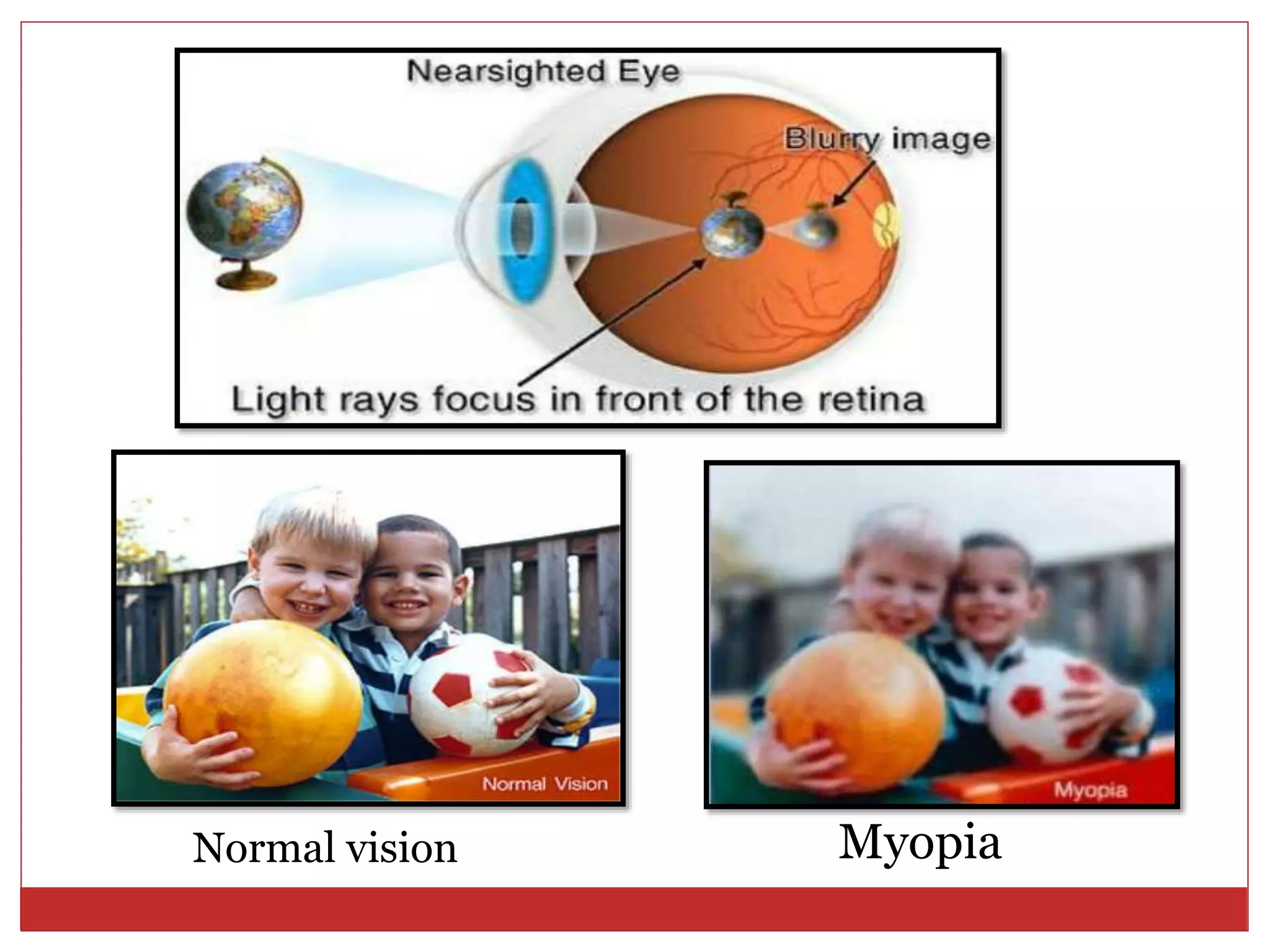
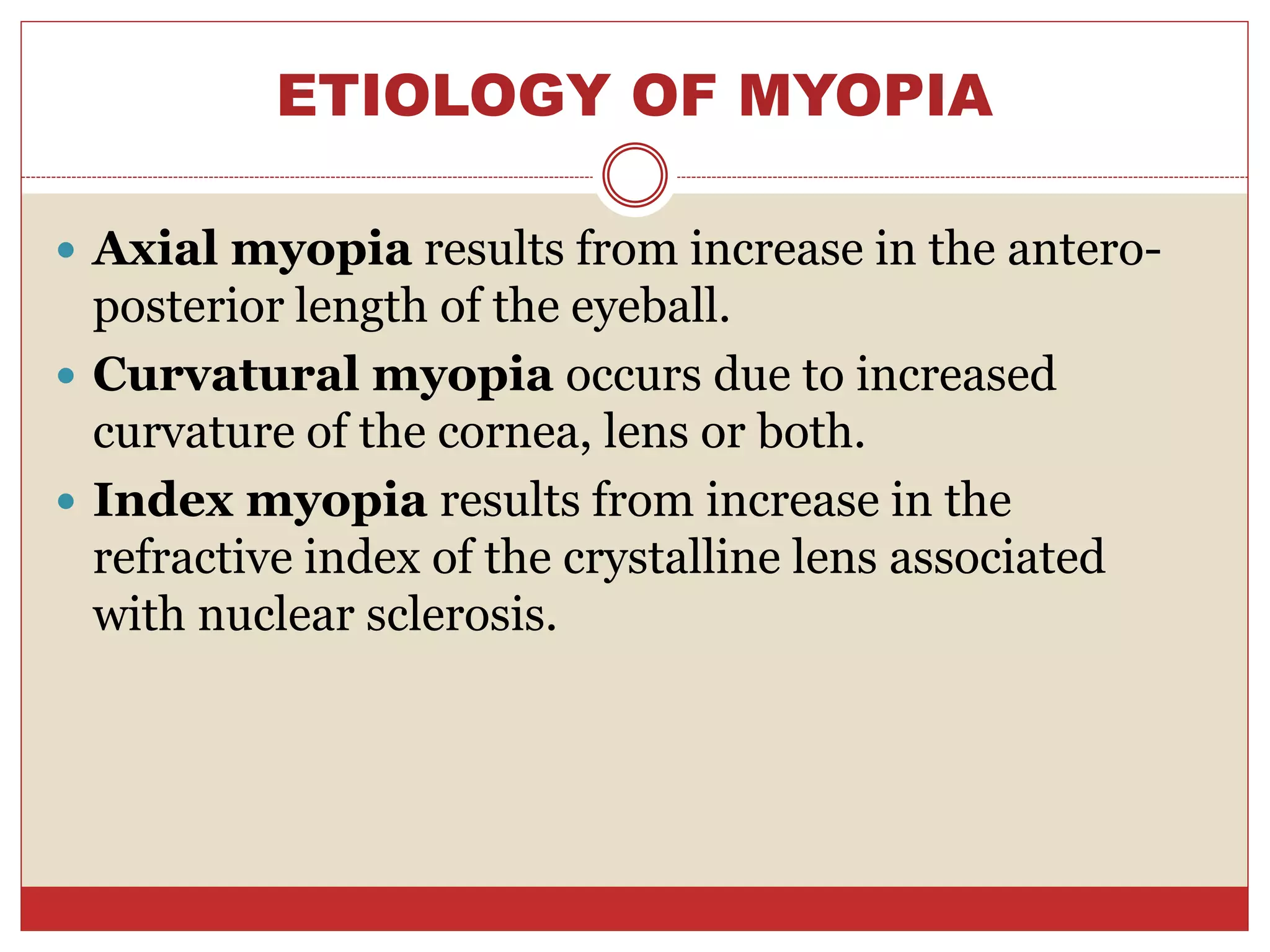
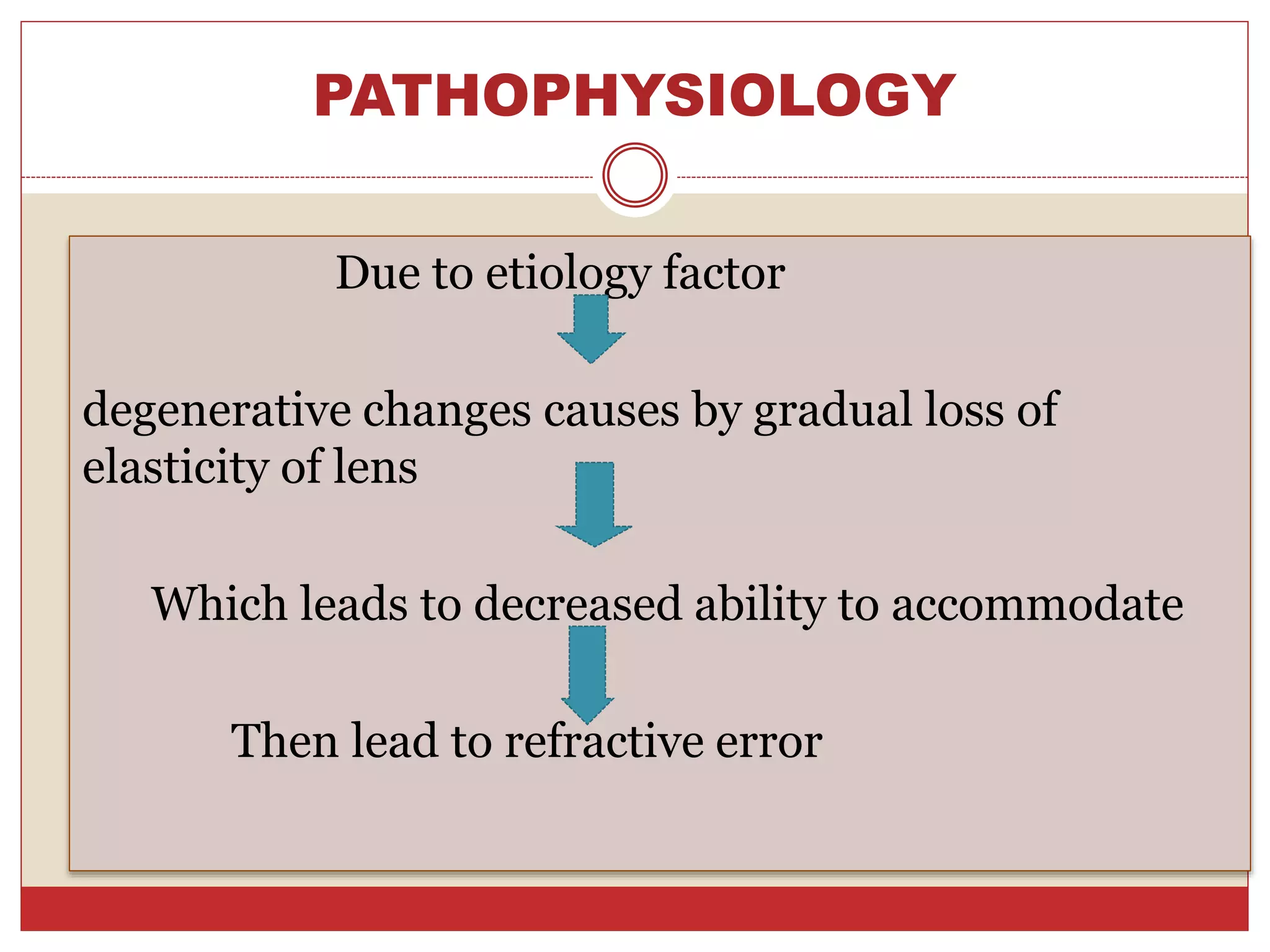
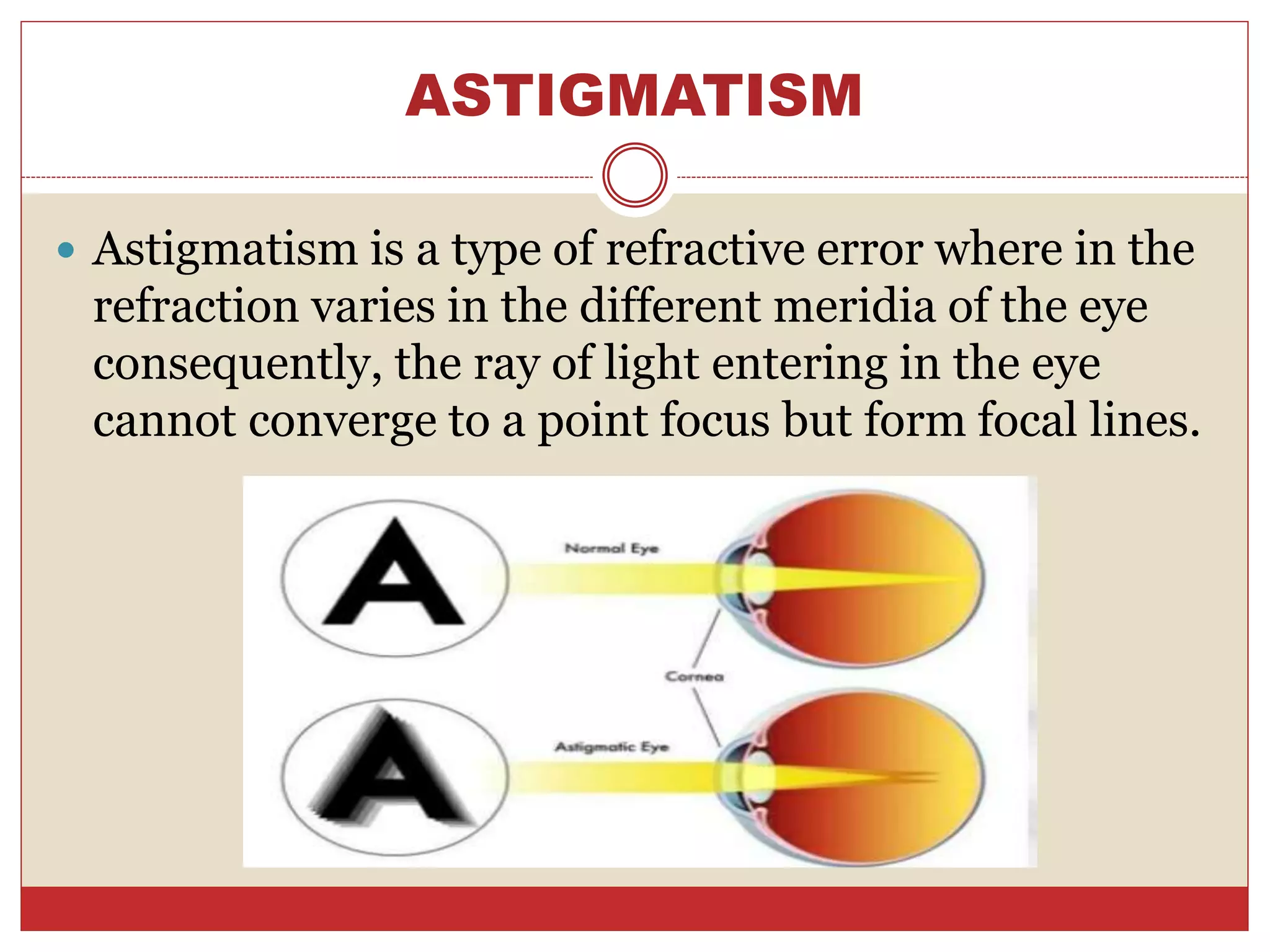
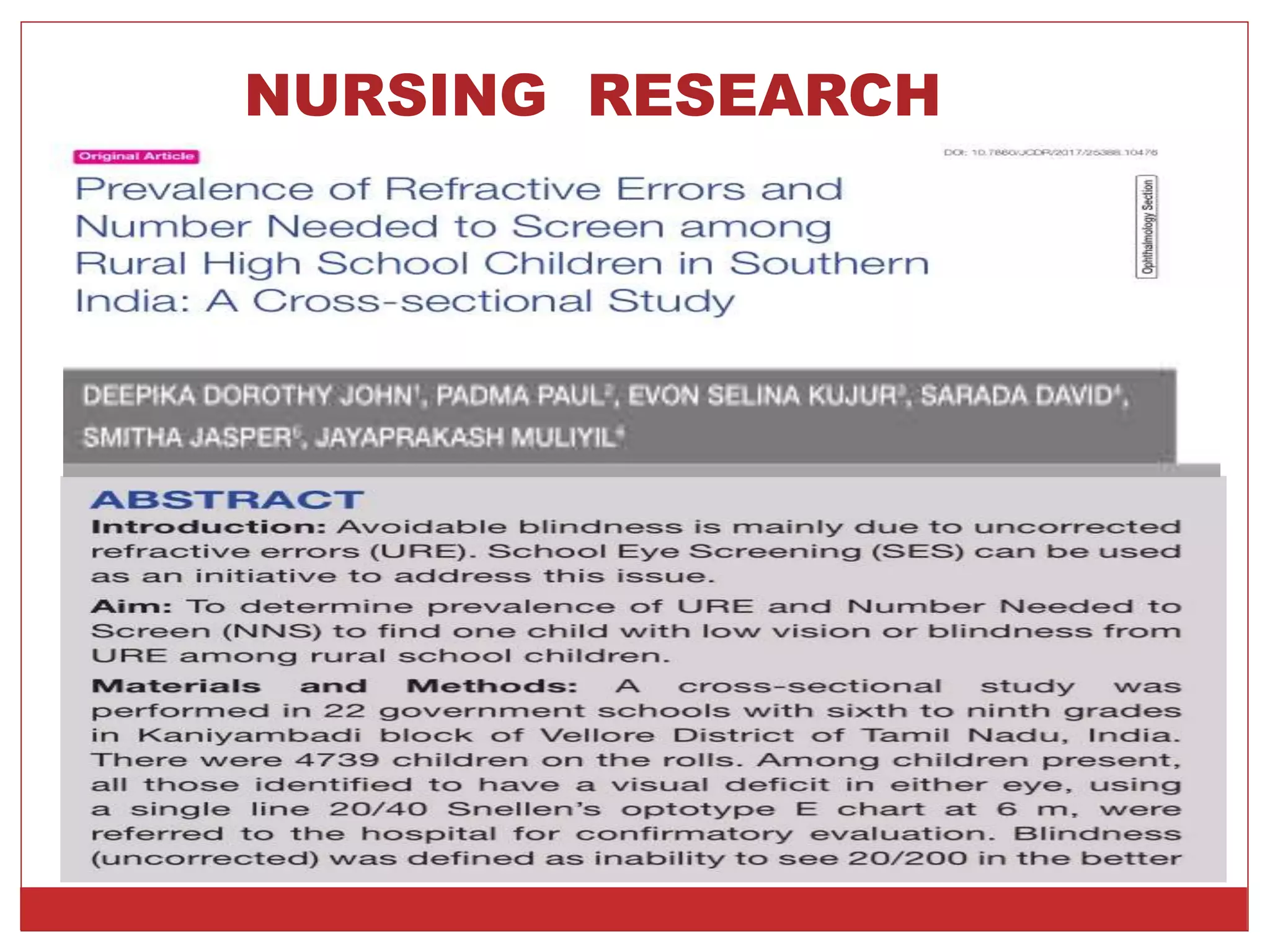
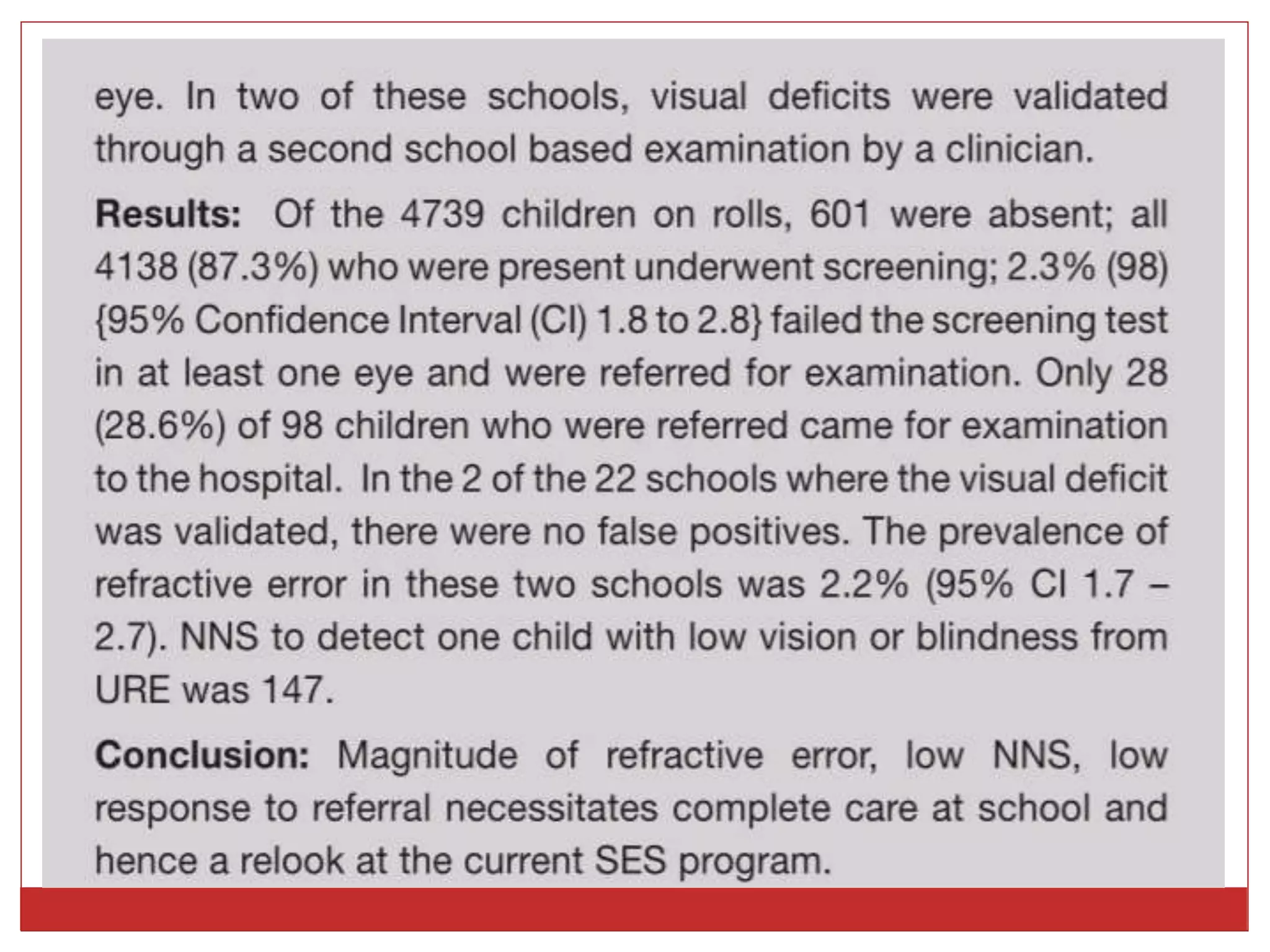
The document discusses refractive errors of the eye, which impair vision due to the inability to focus light correctly on the retina. It elaborates on various types of refractive errors, including myopia, hyperopia, astigmatism, and presbyopia, their etiologies, clinical manifestations, and management options. Additionally, it outlines diagnostic evaluations and nursing management relevant to treatment and care for patients with refractive disorders.