Downloaded 253 times
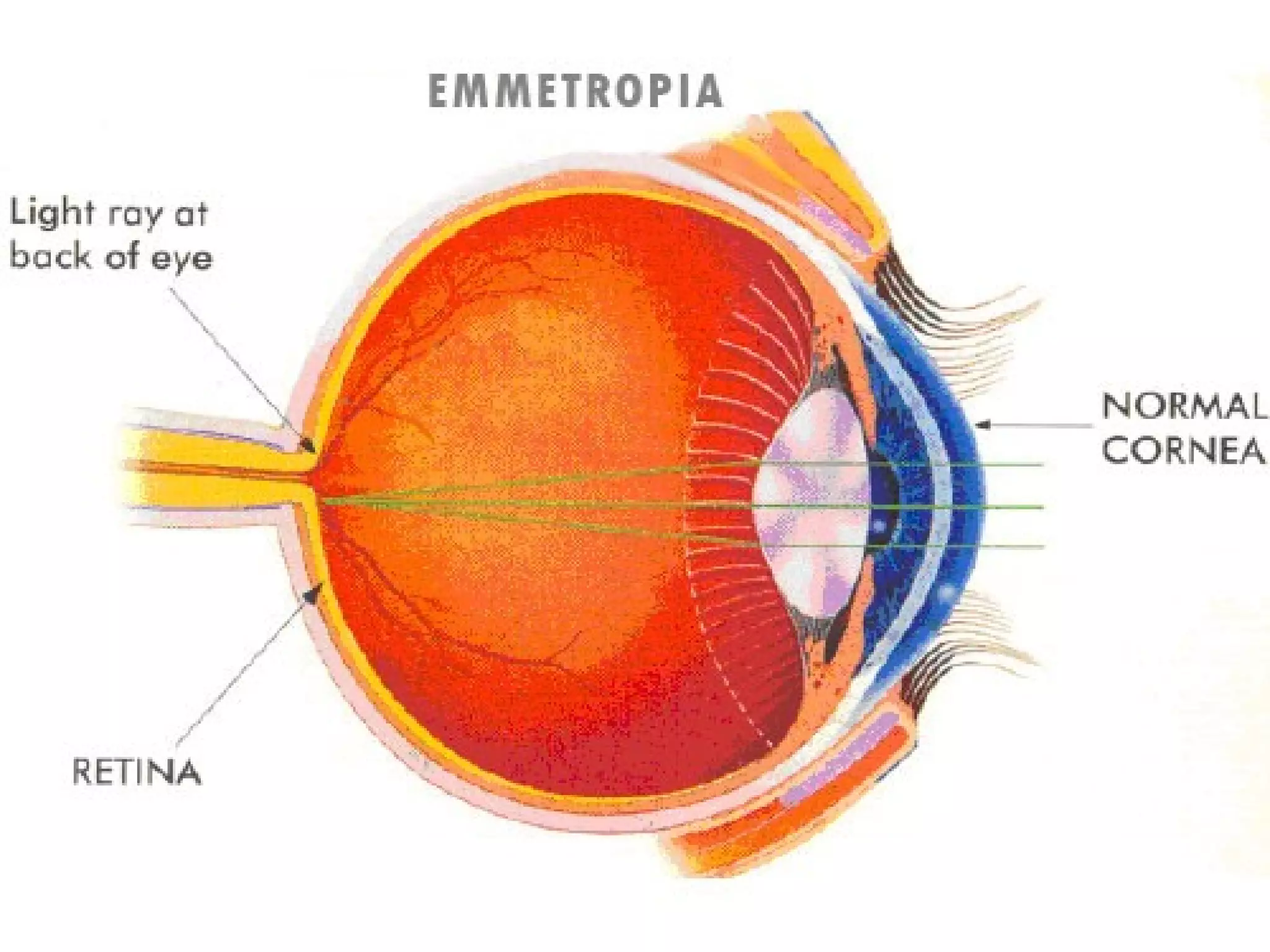
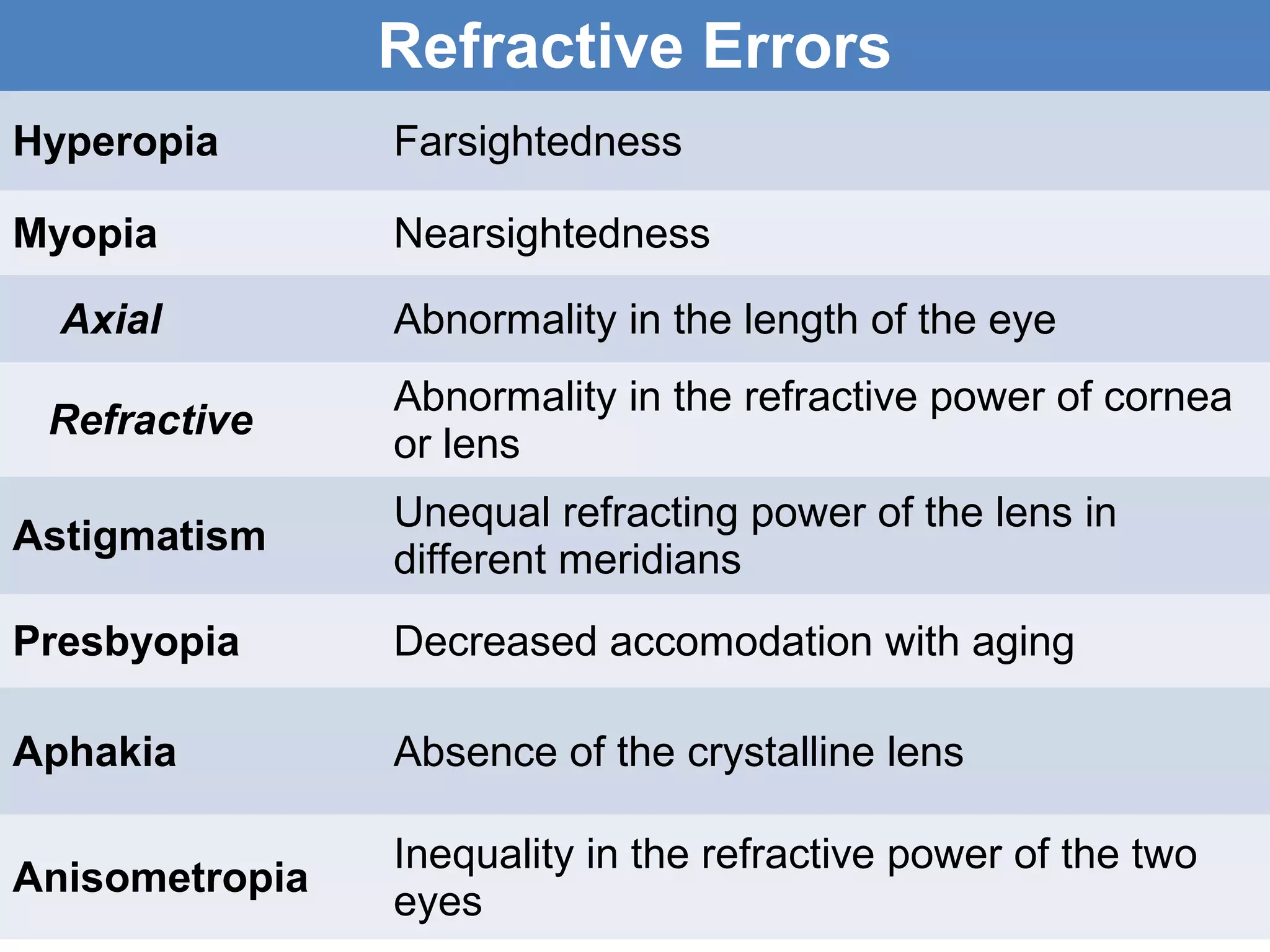
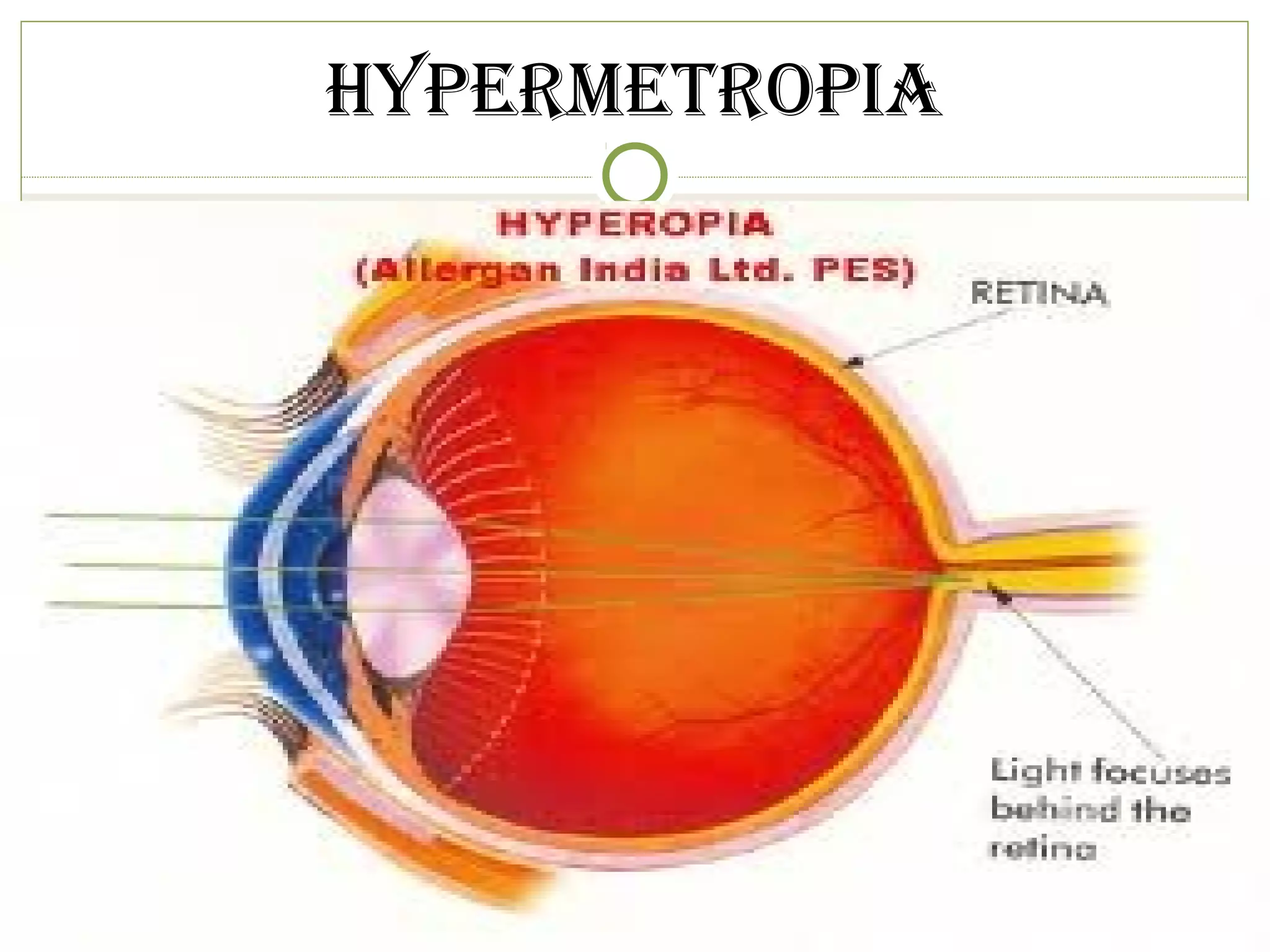
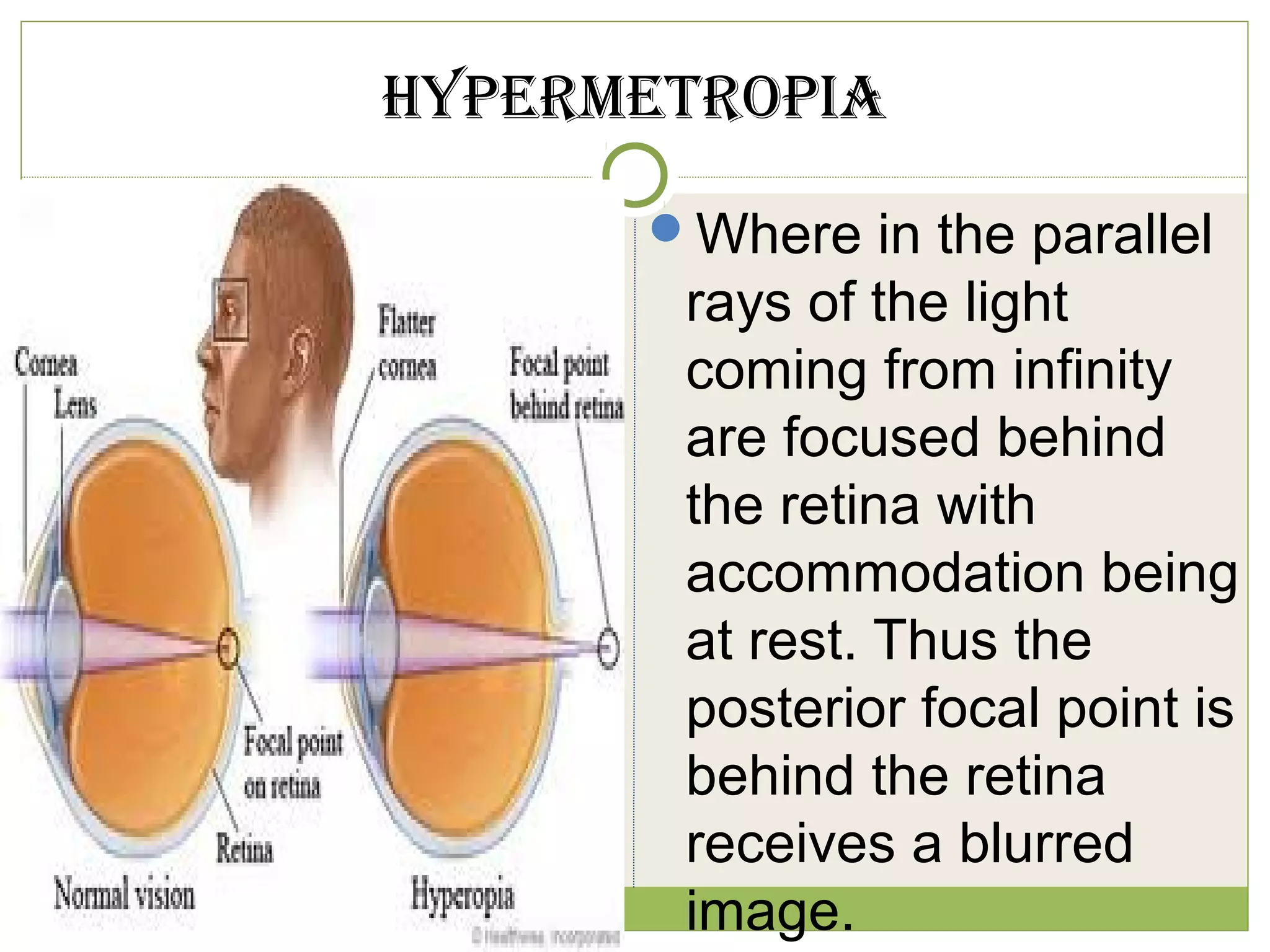
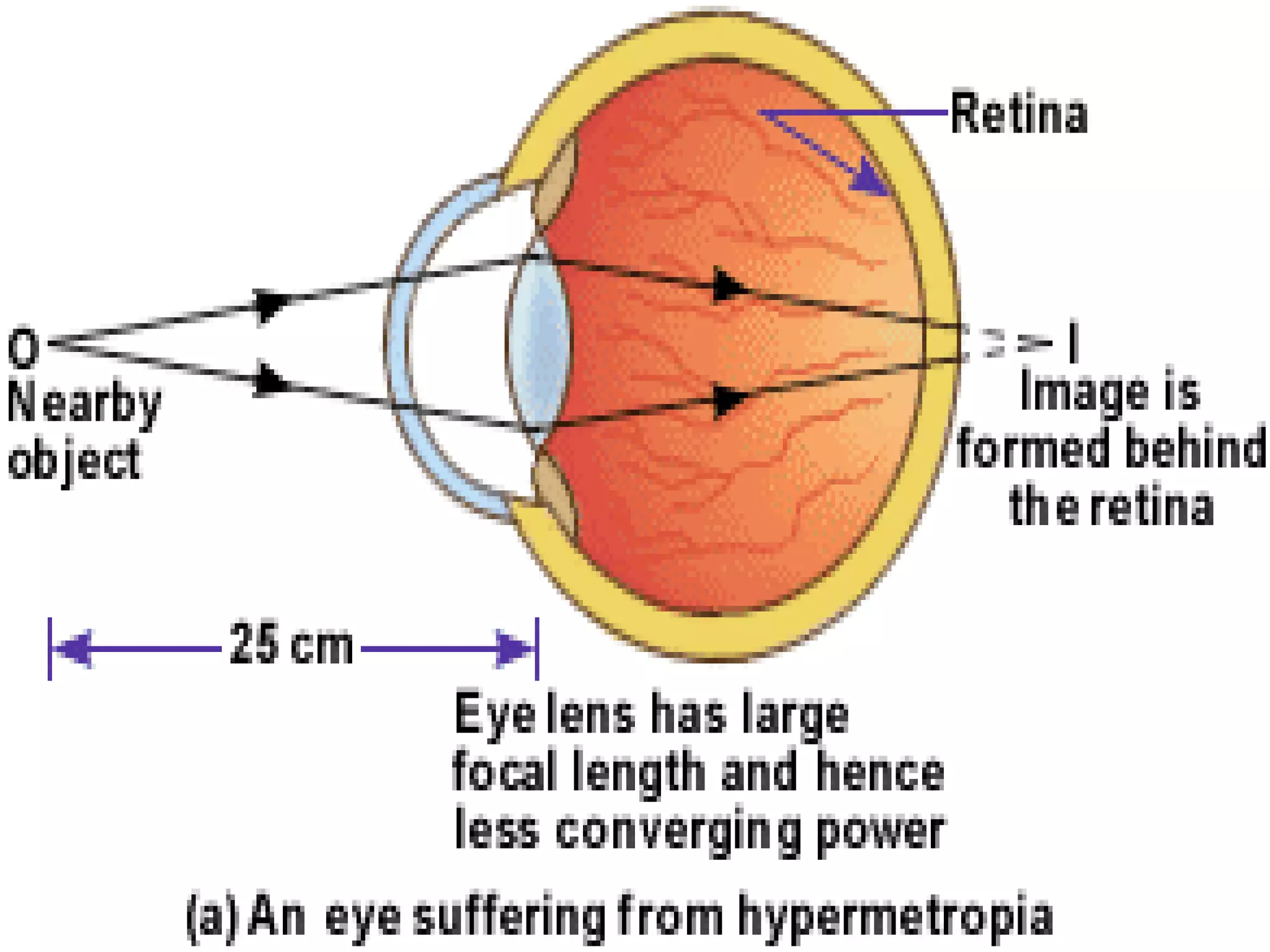

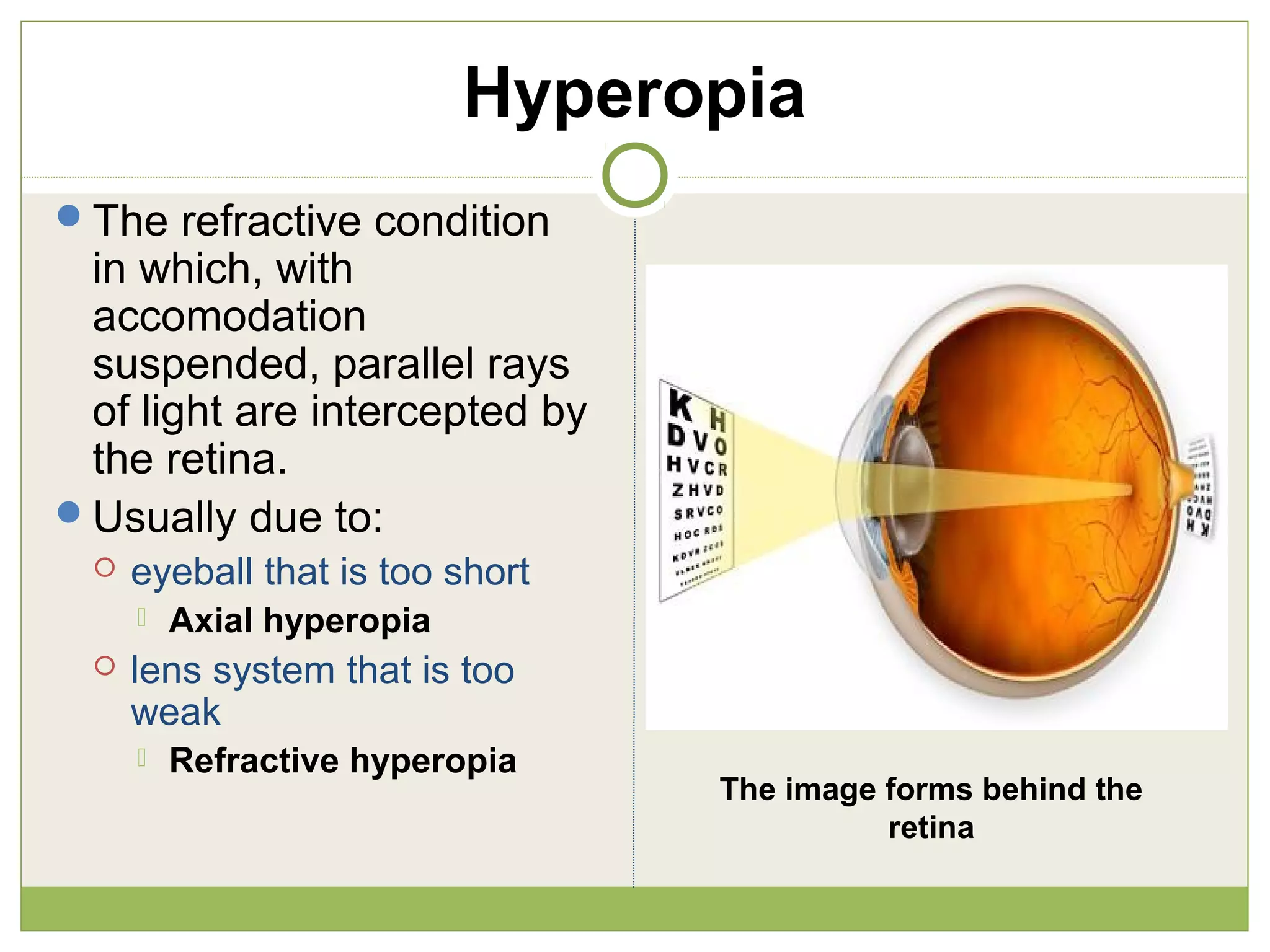

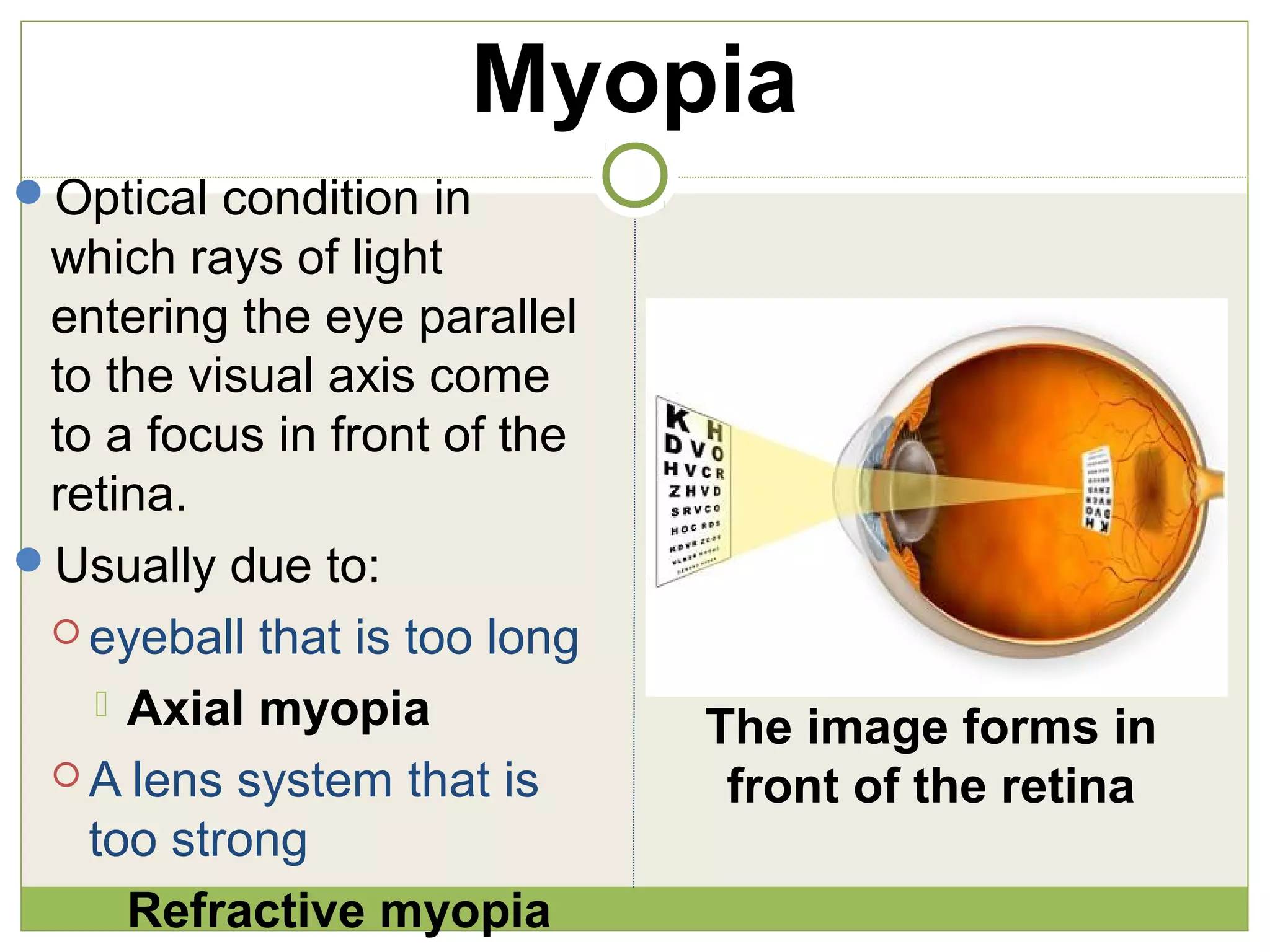
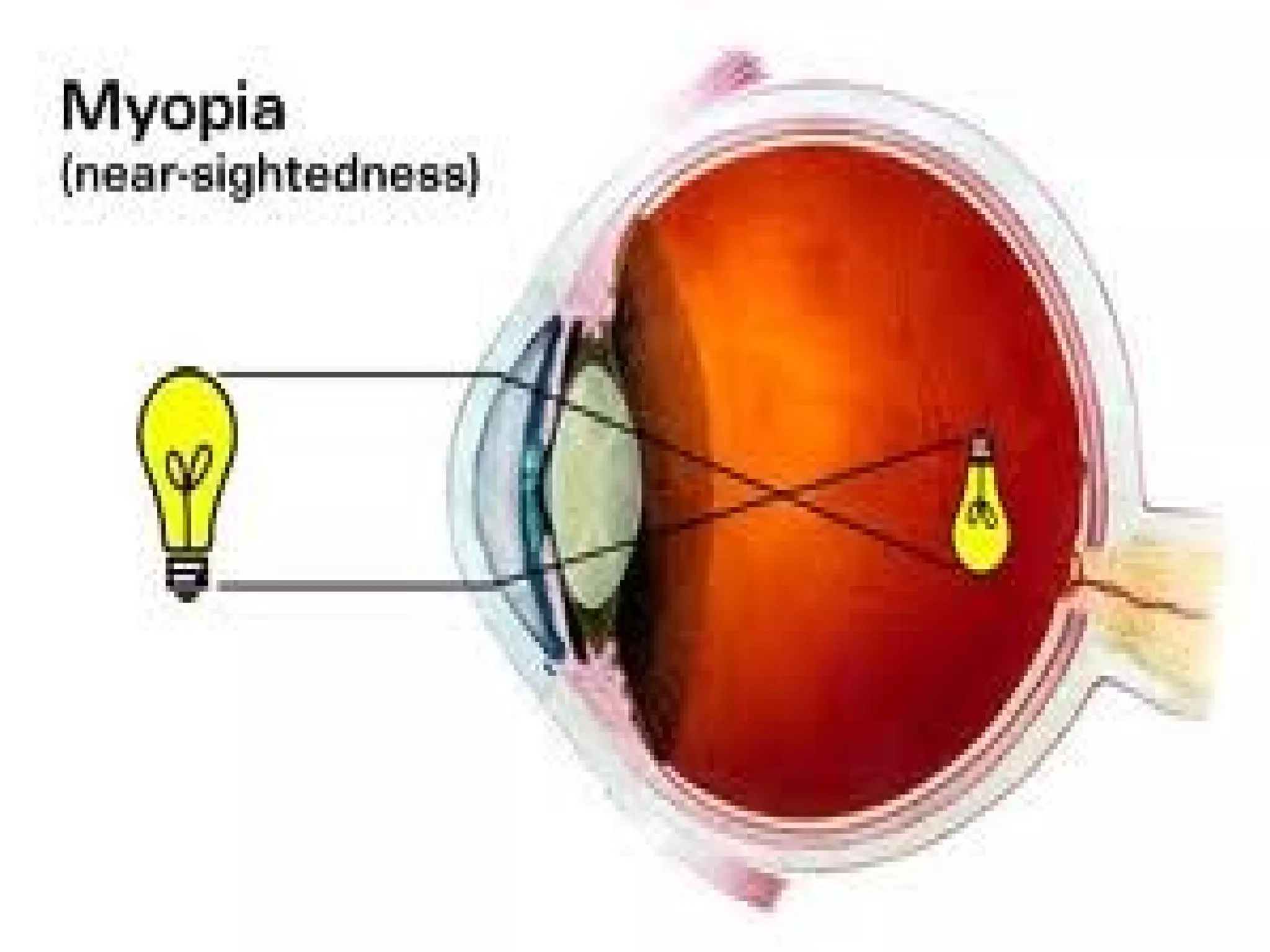
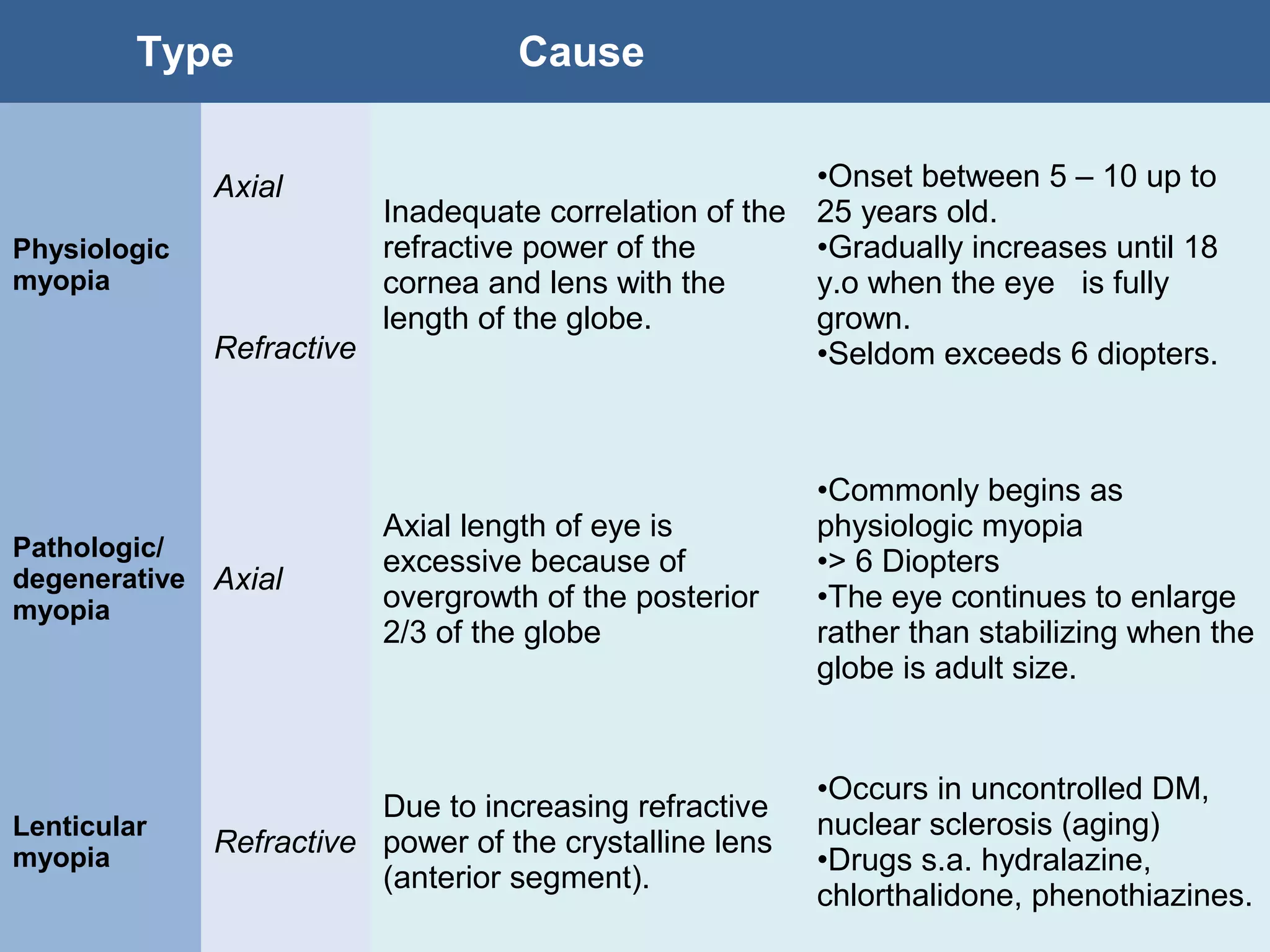
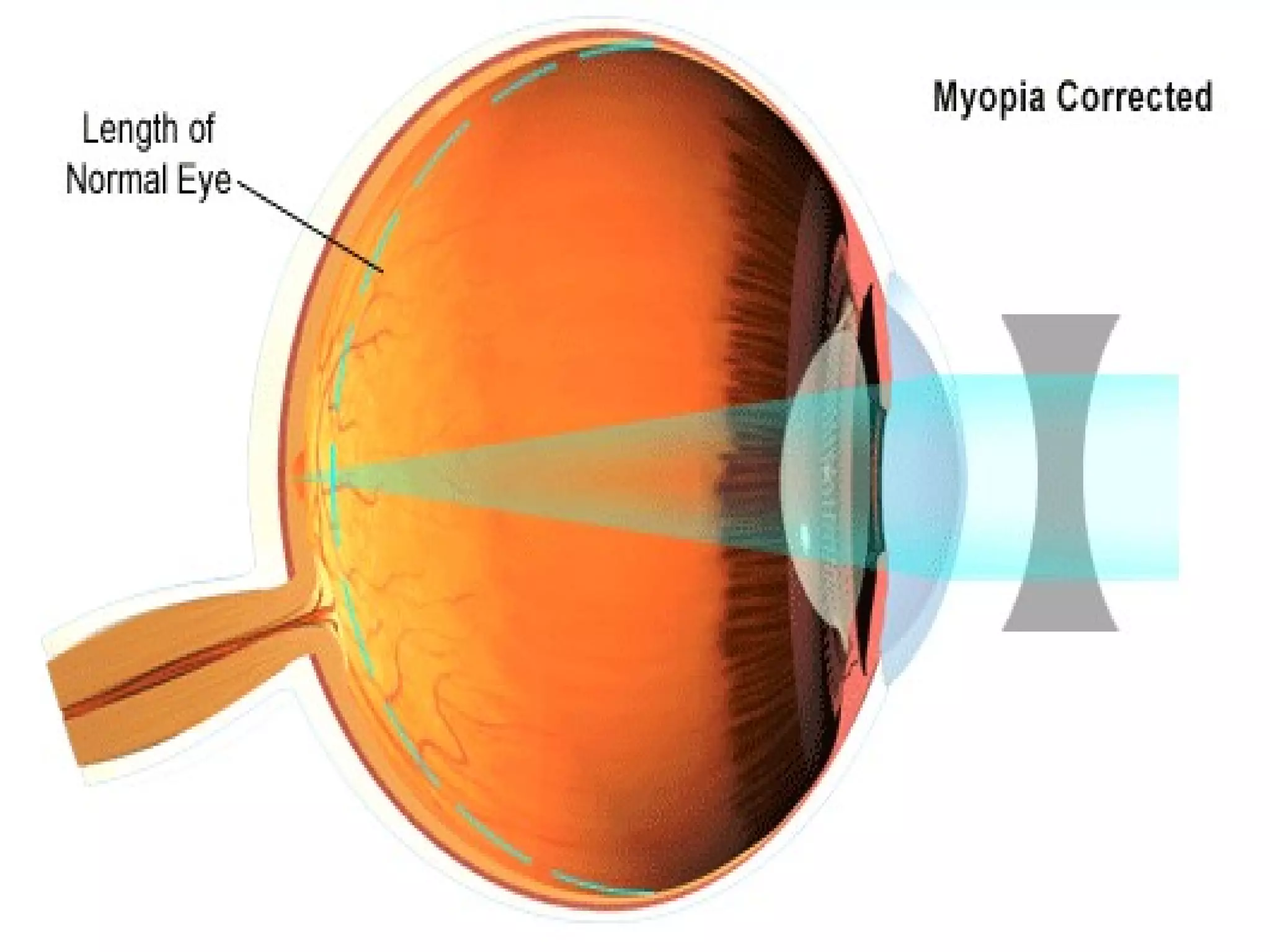
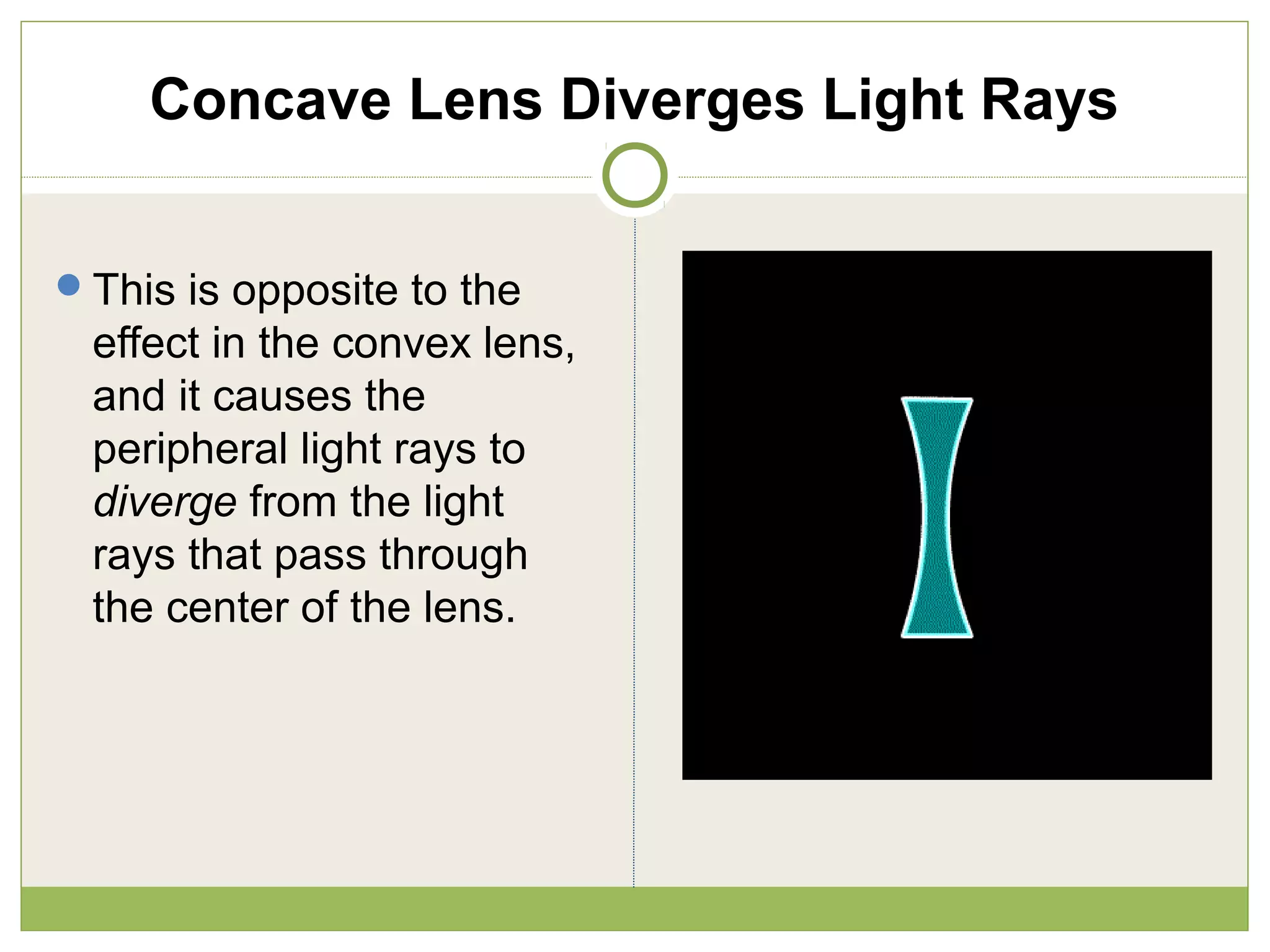
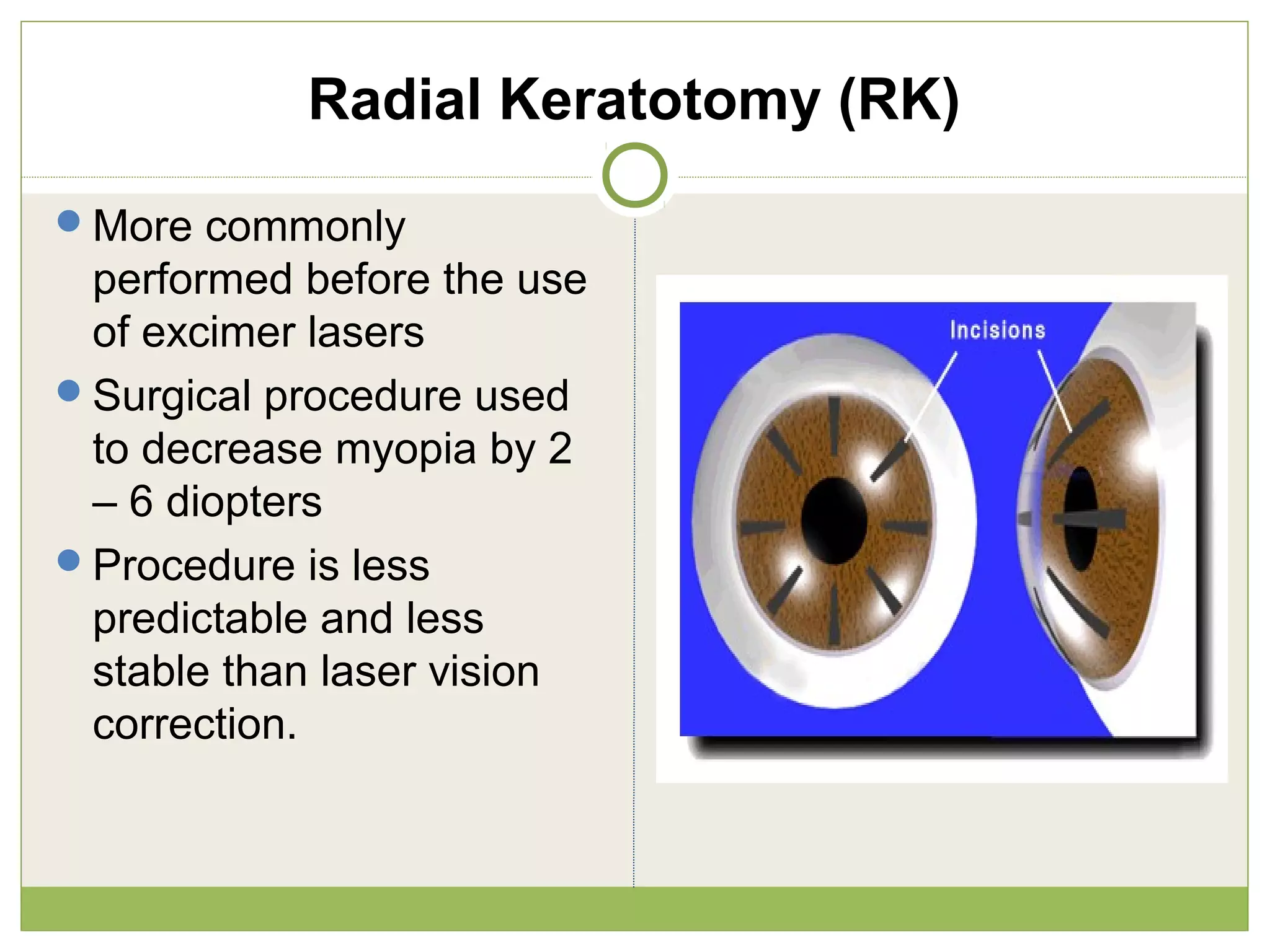
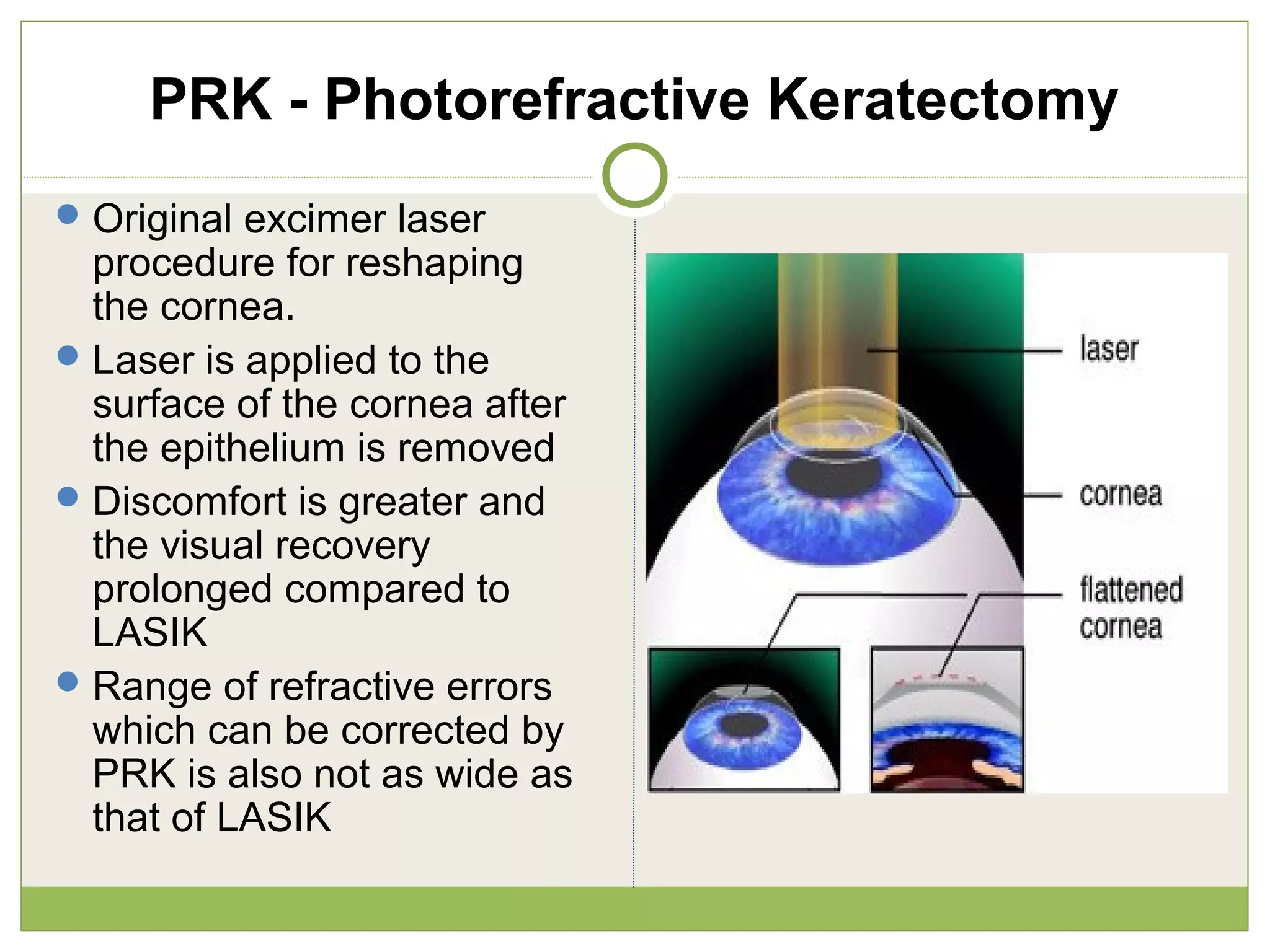
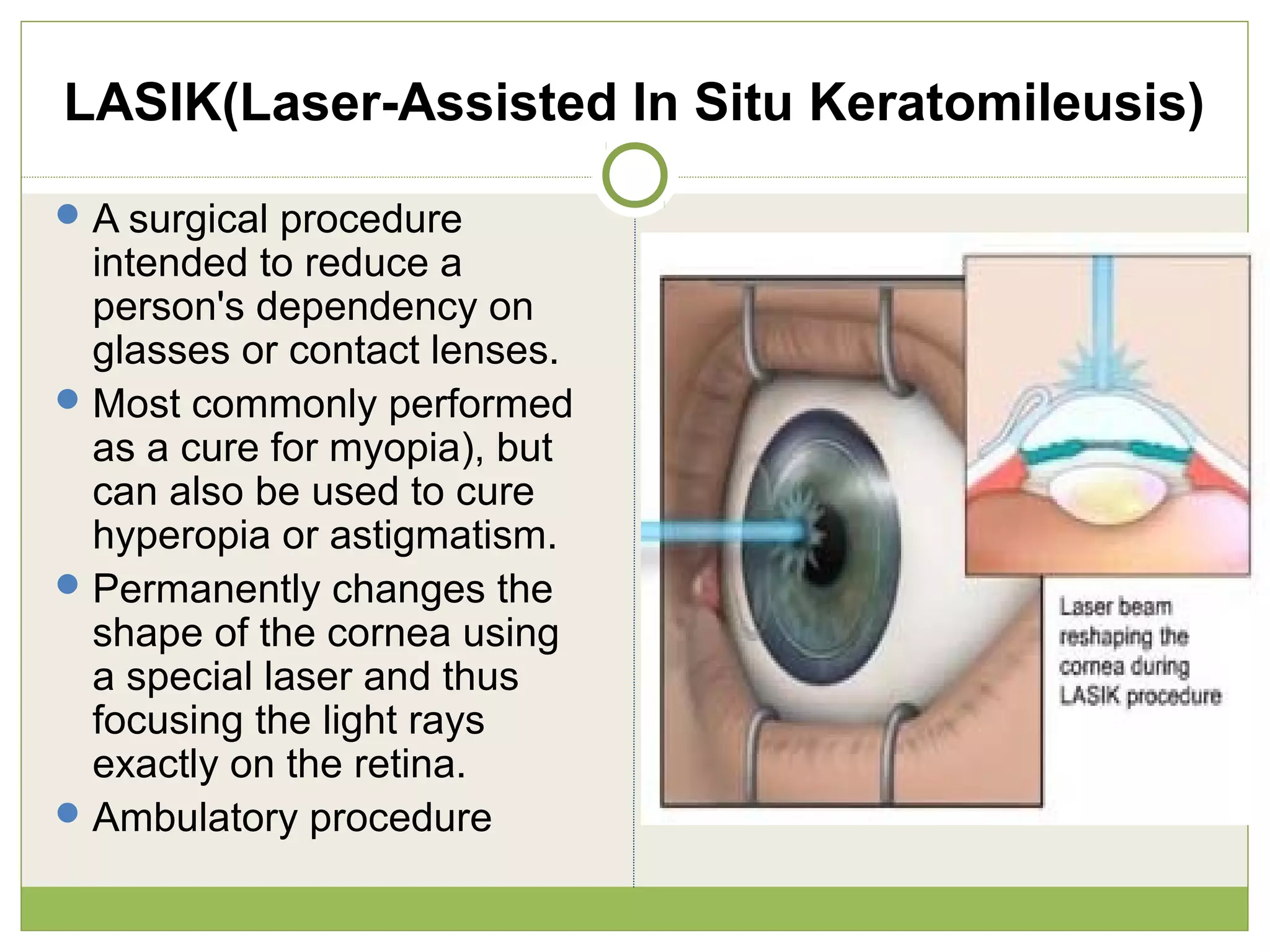
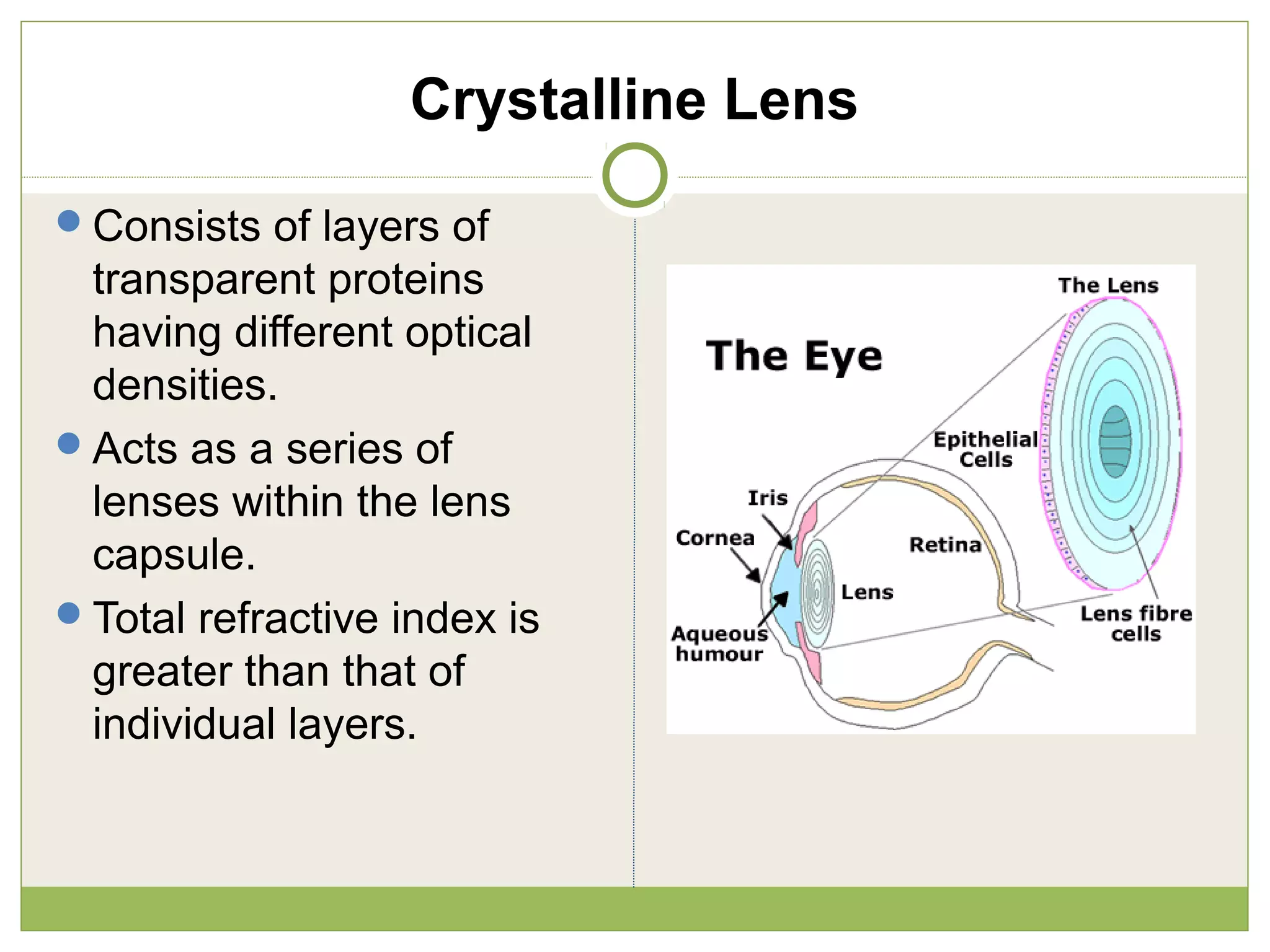
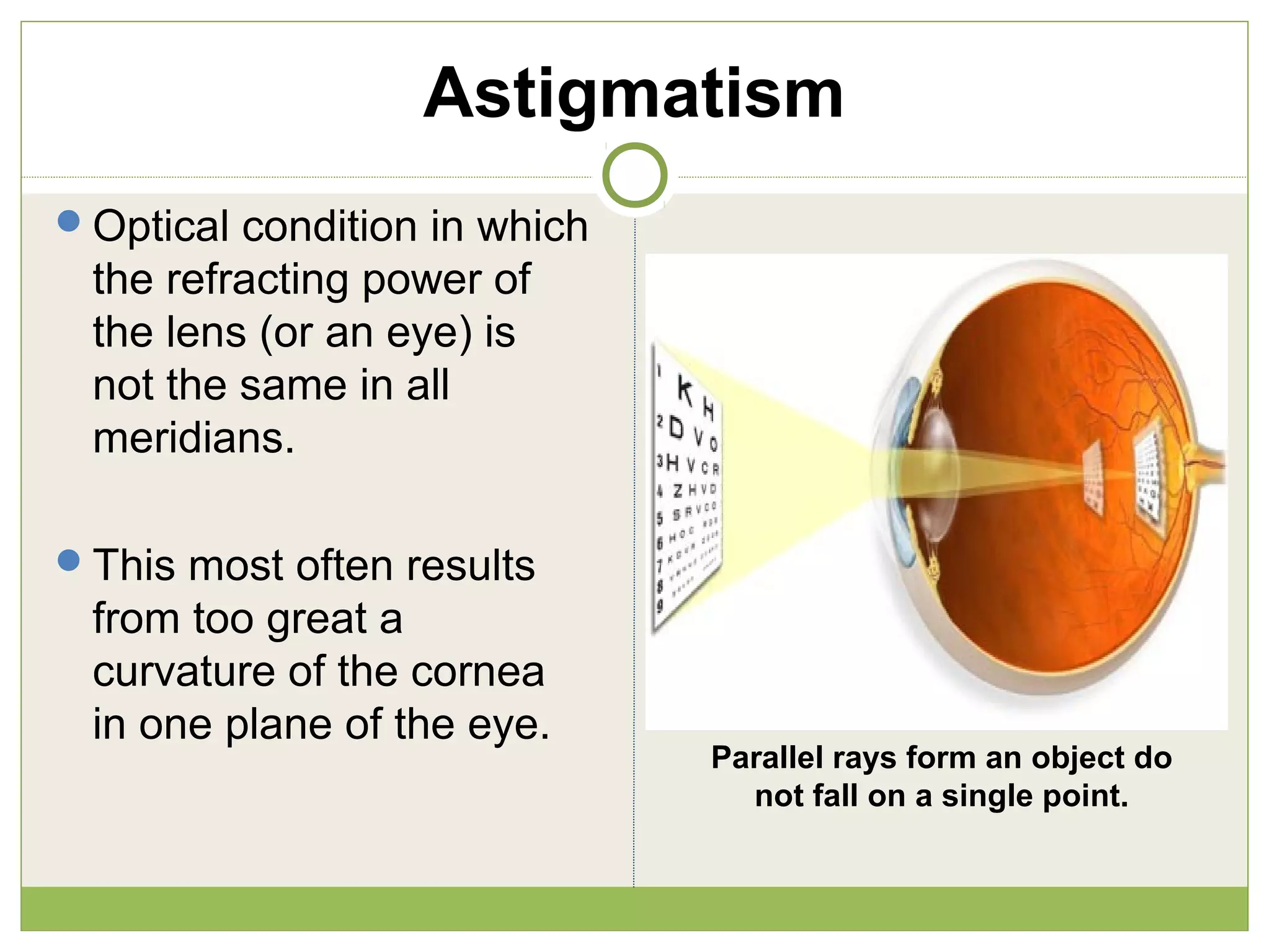
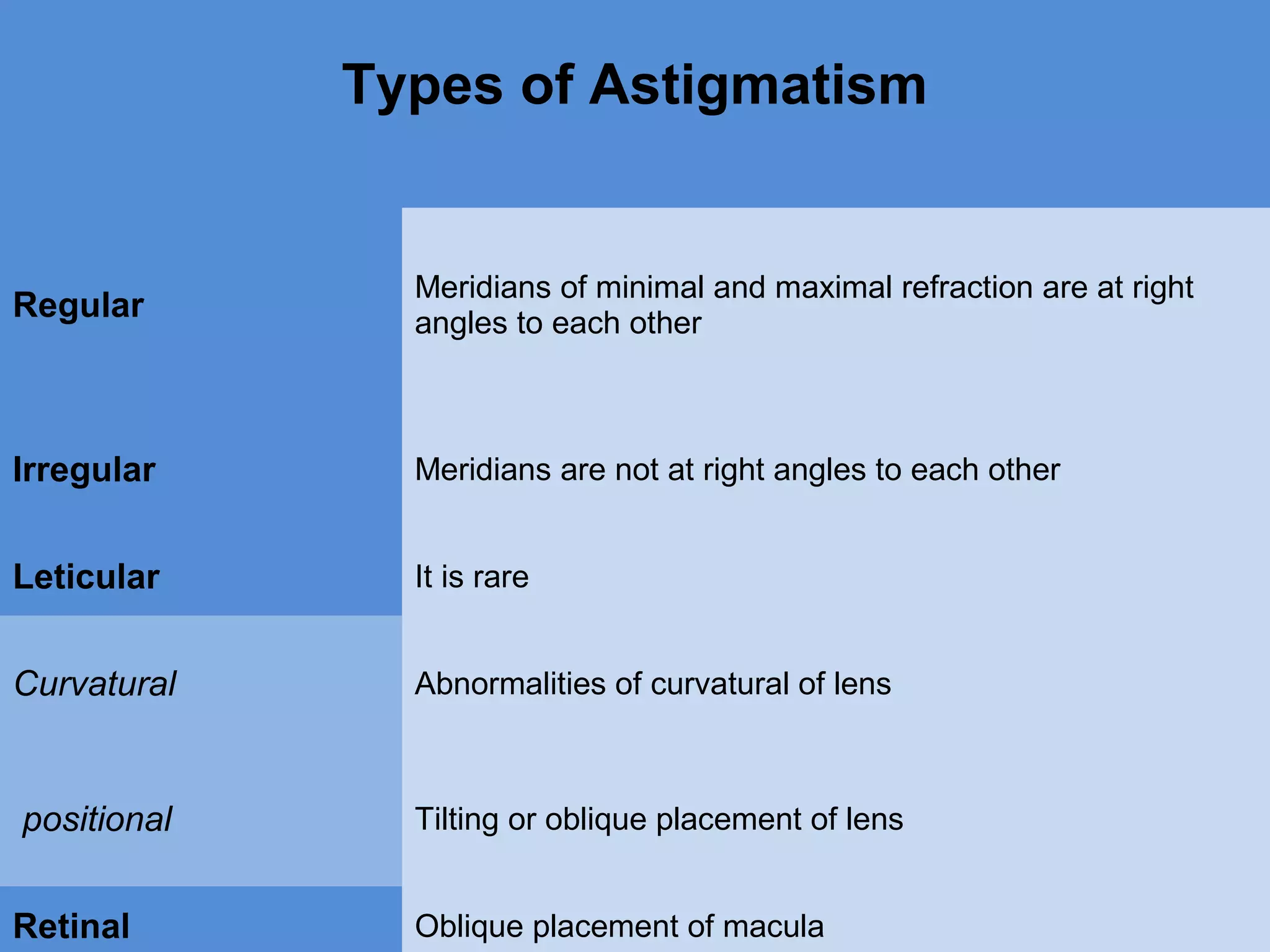
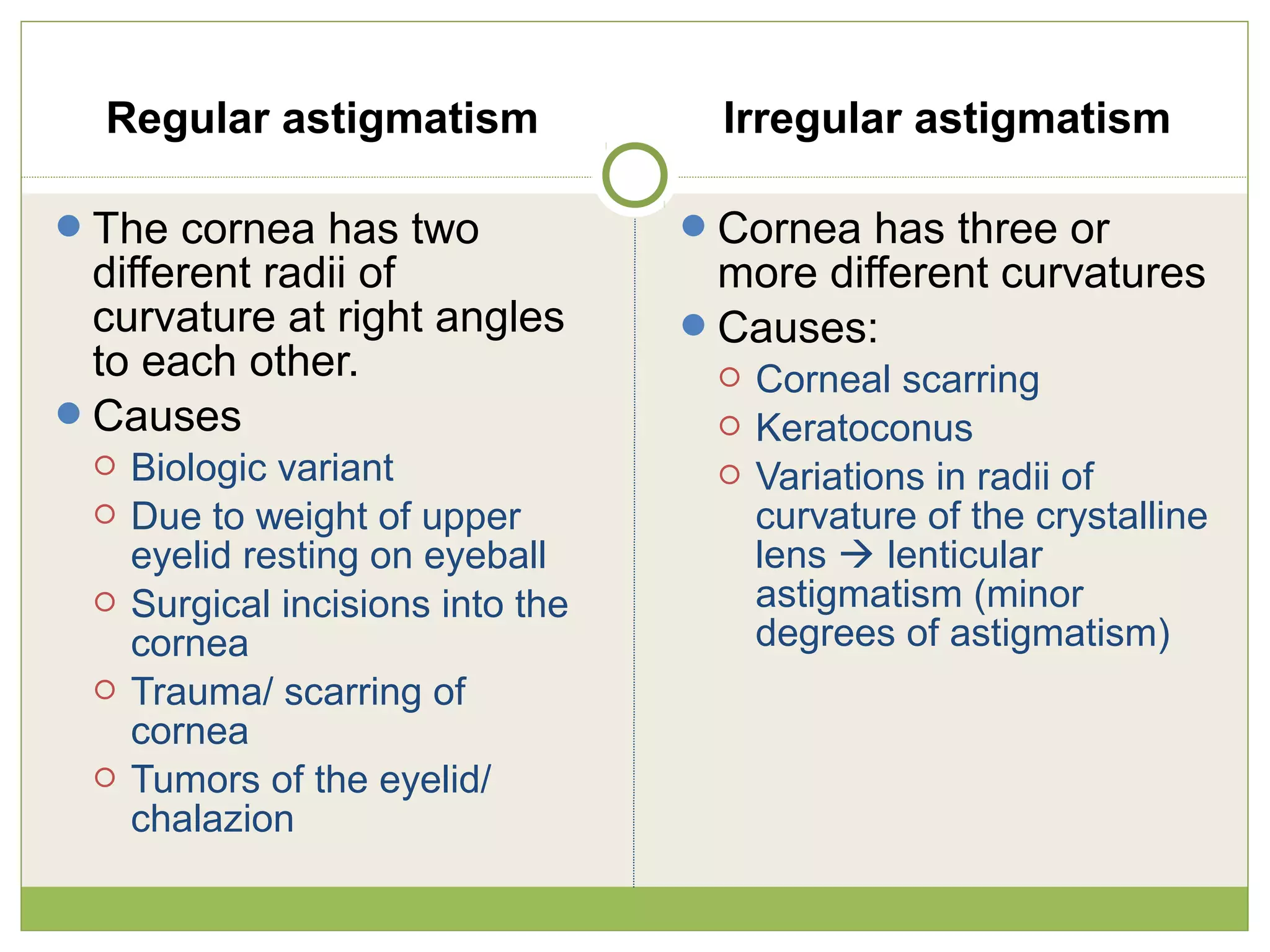
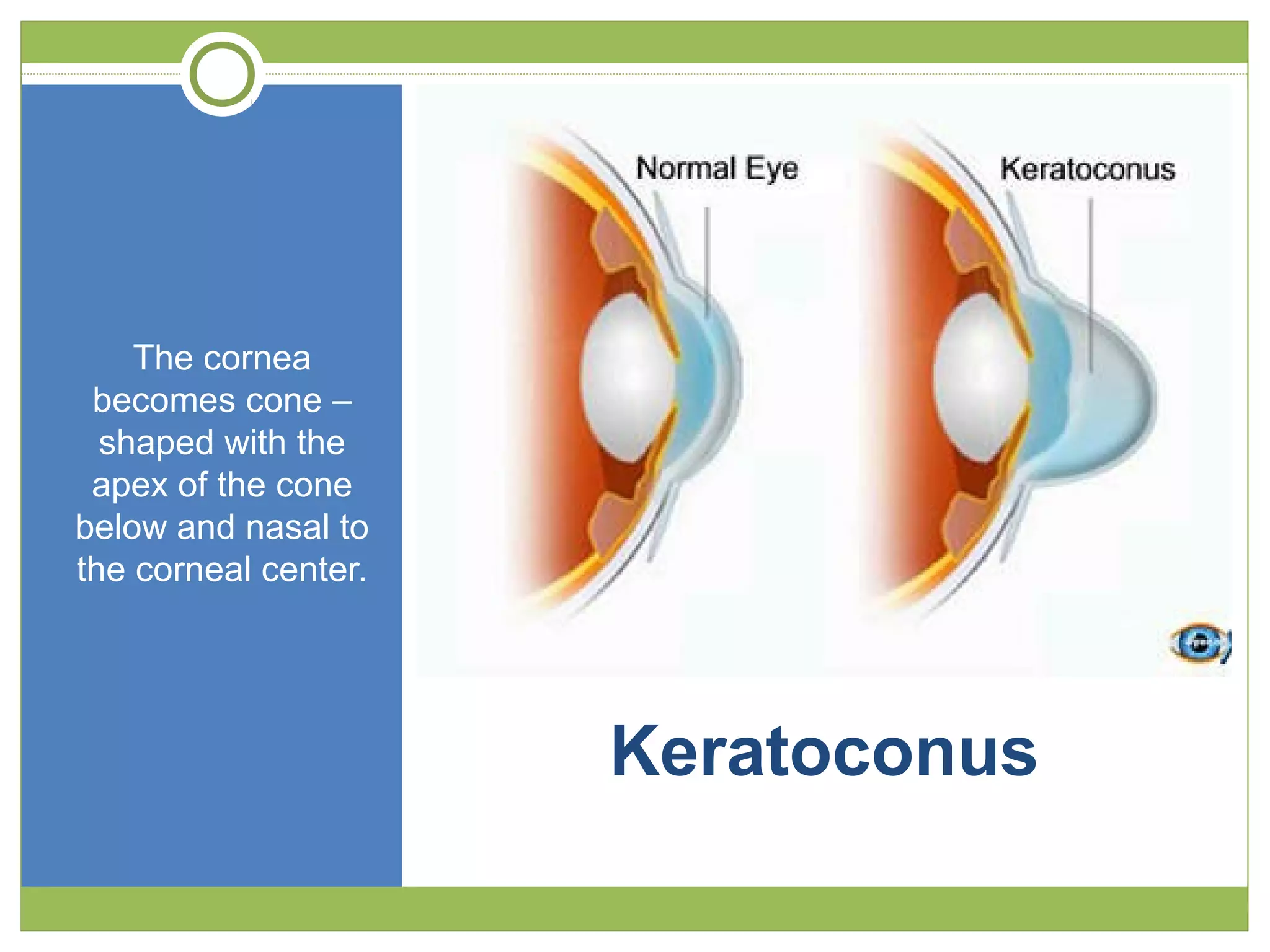
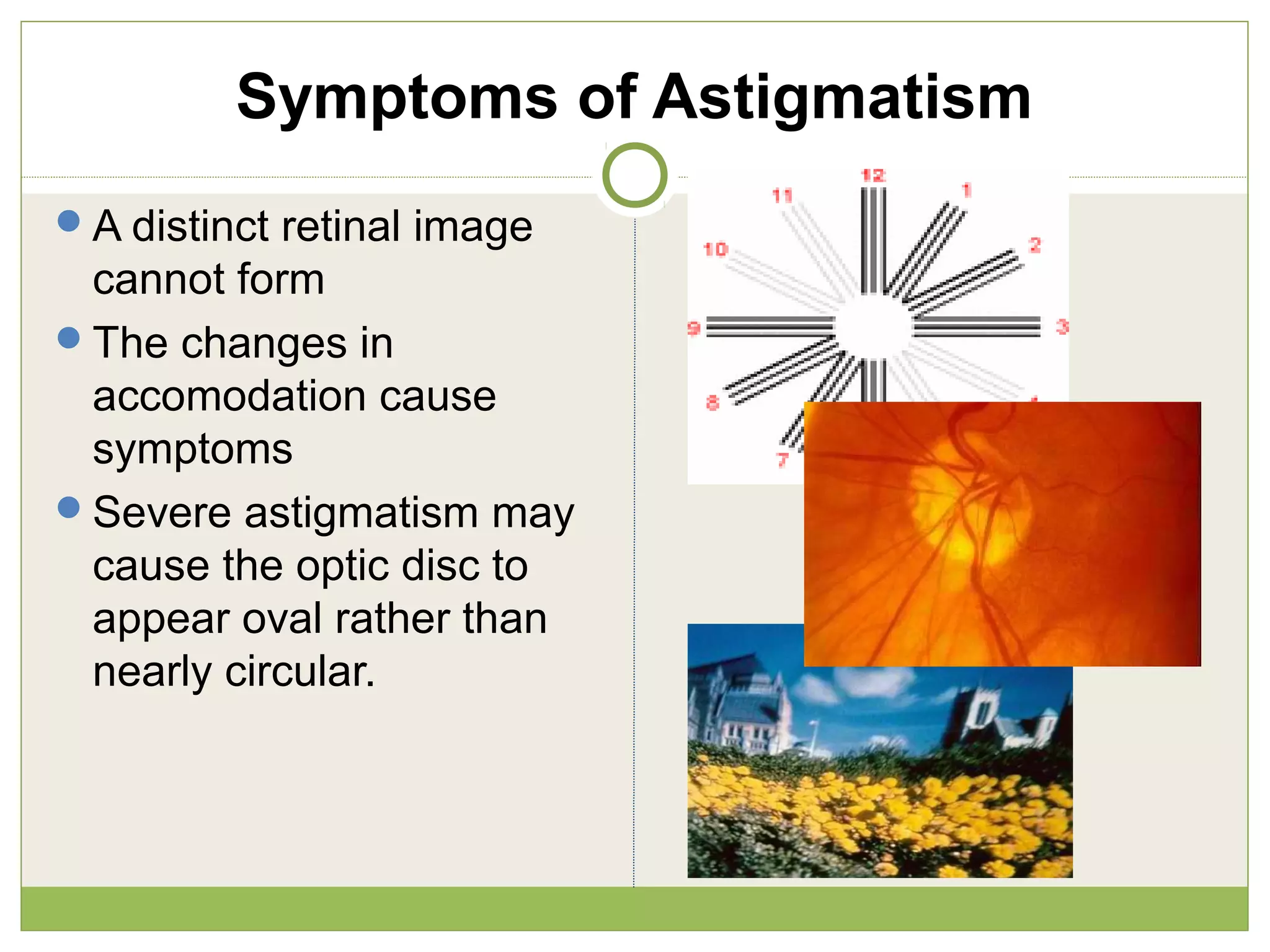

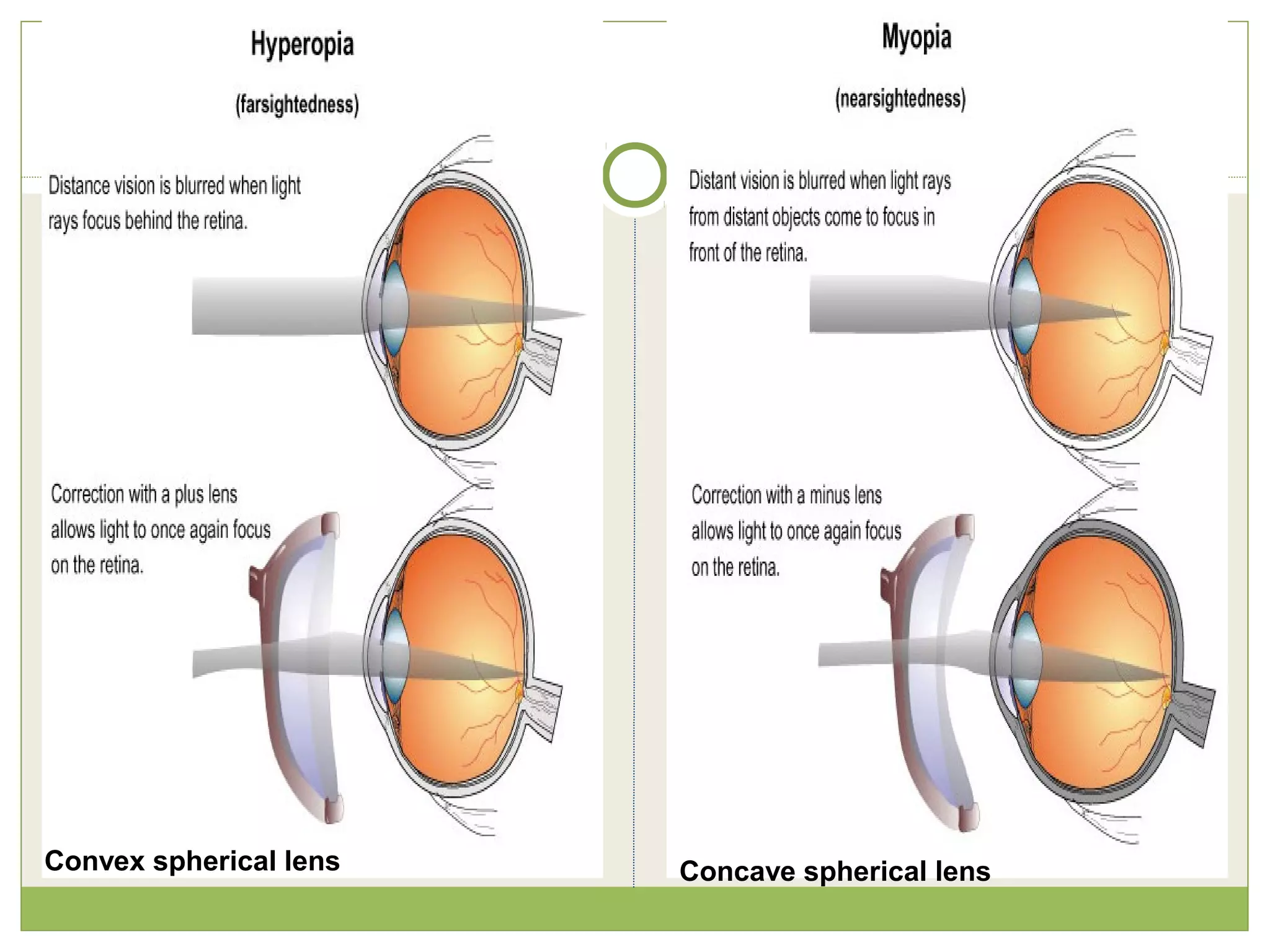
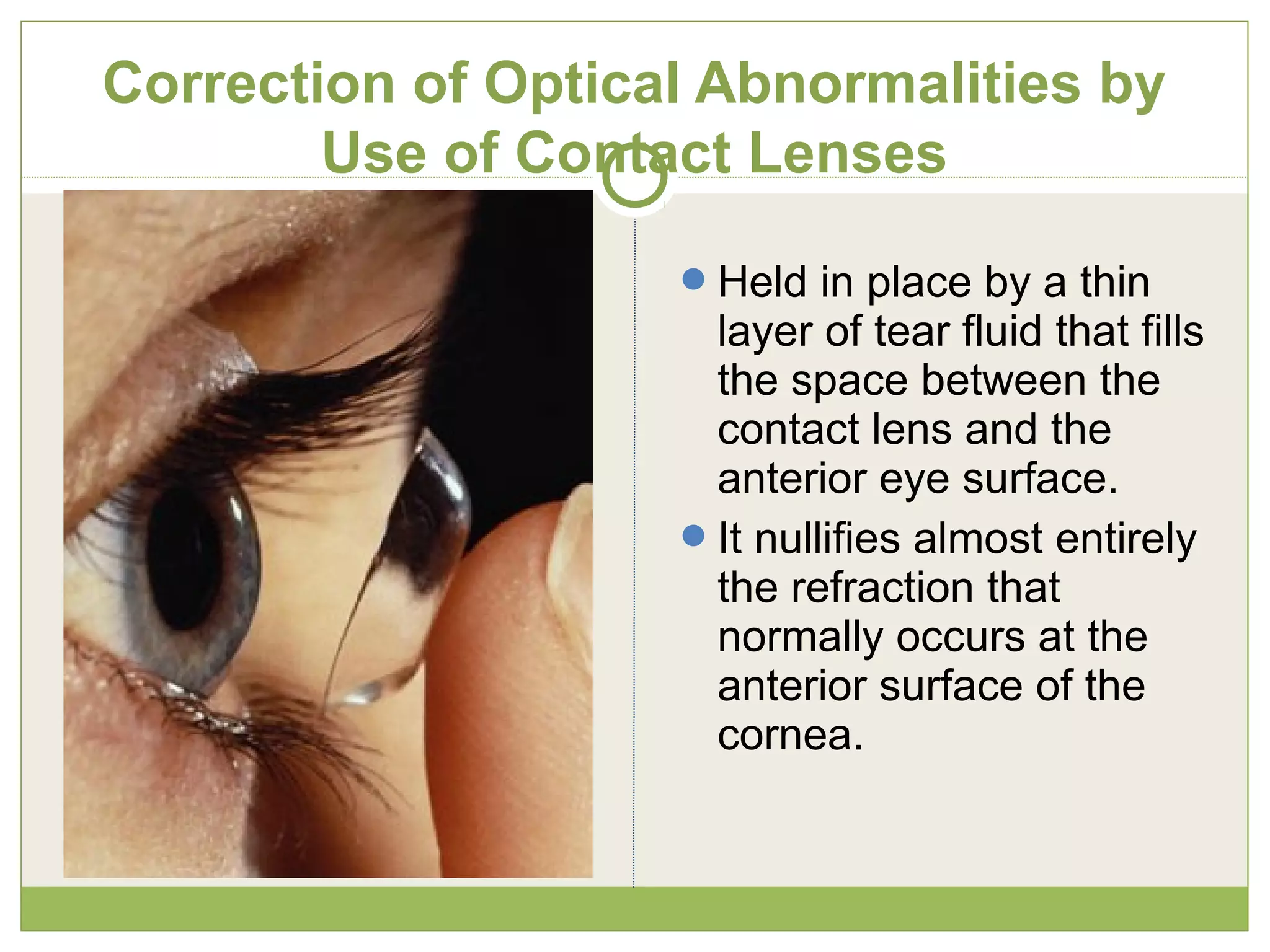
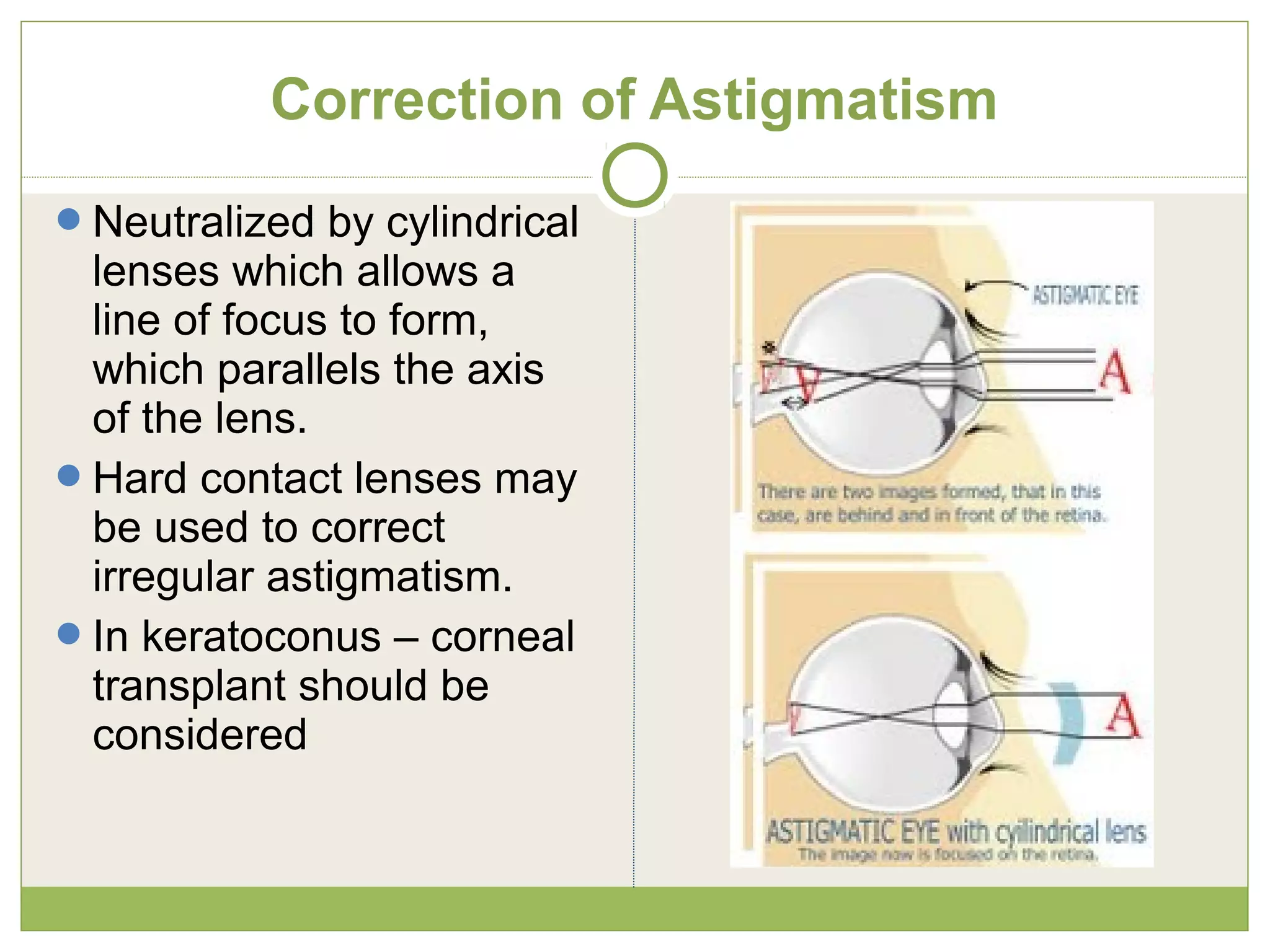
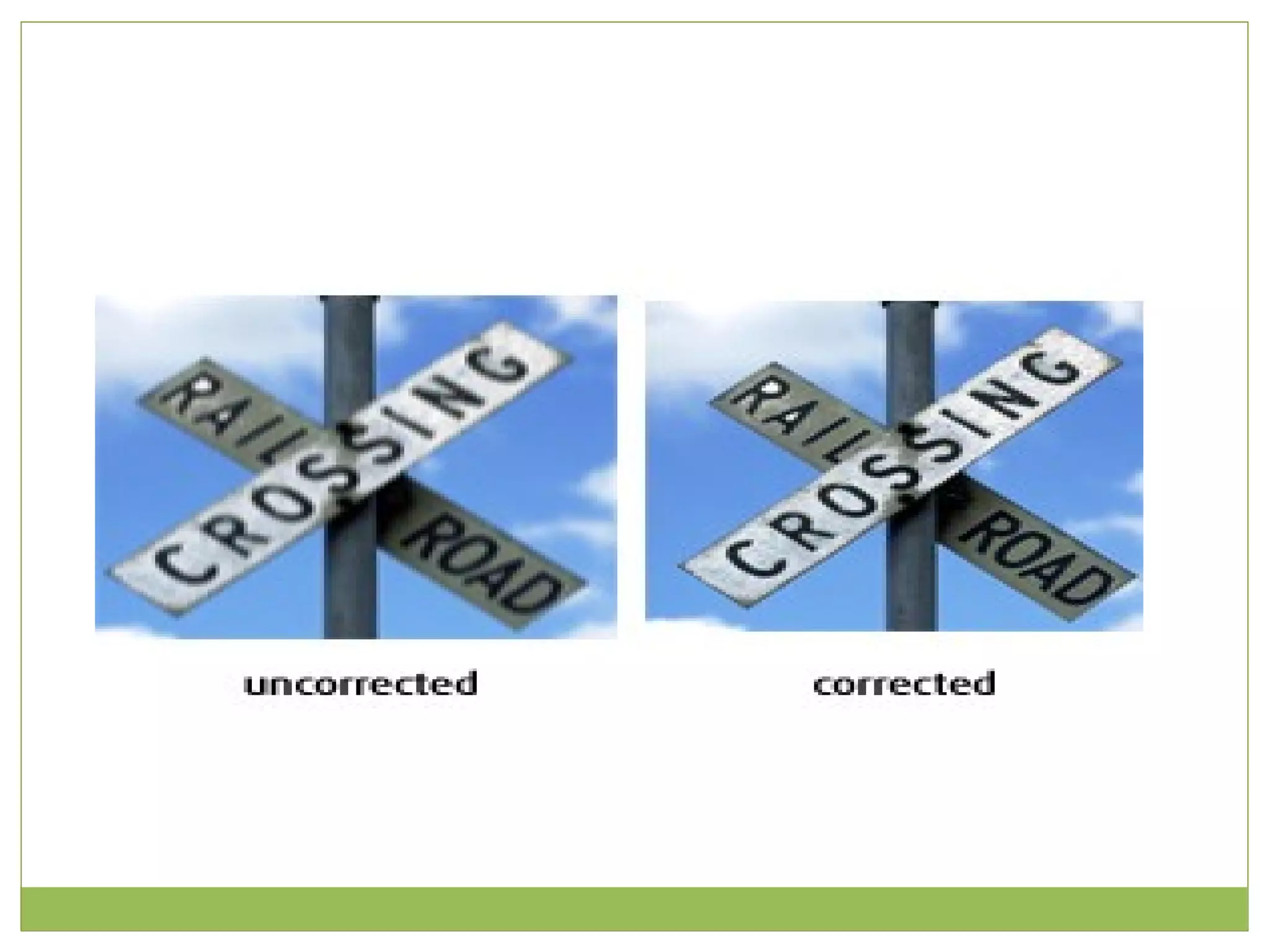
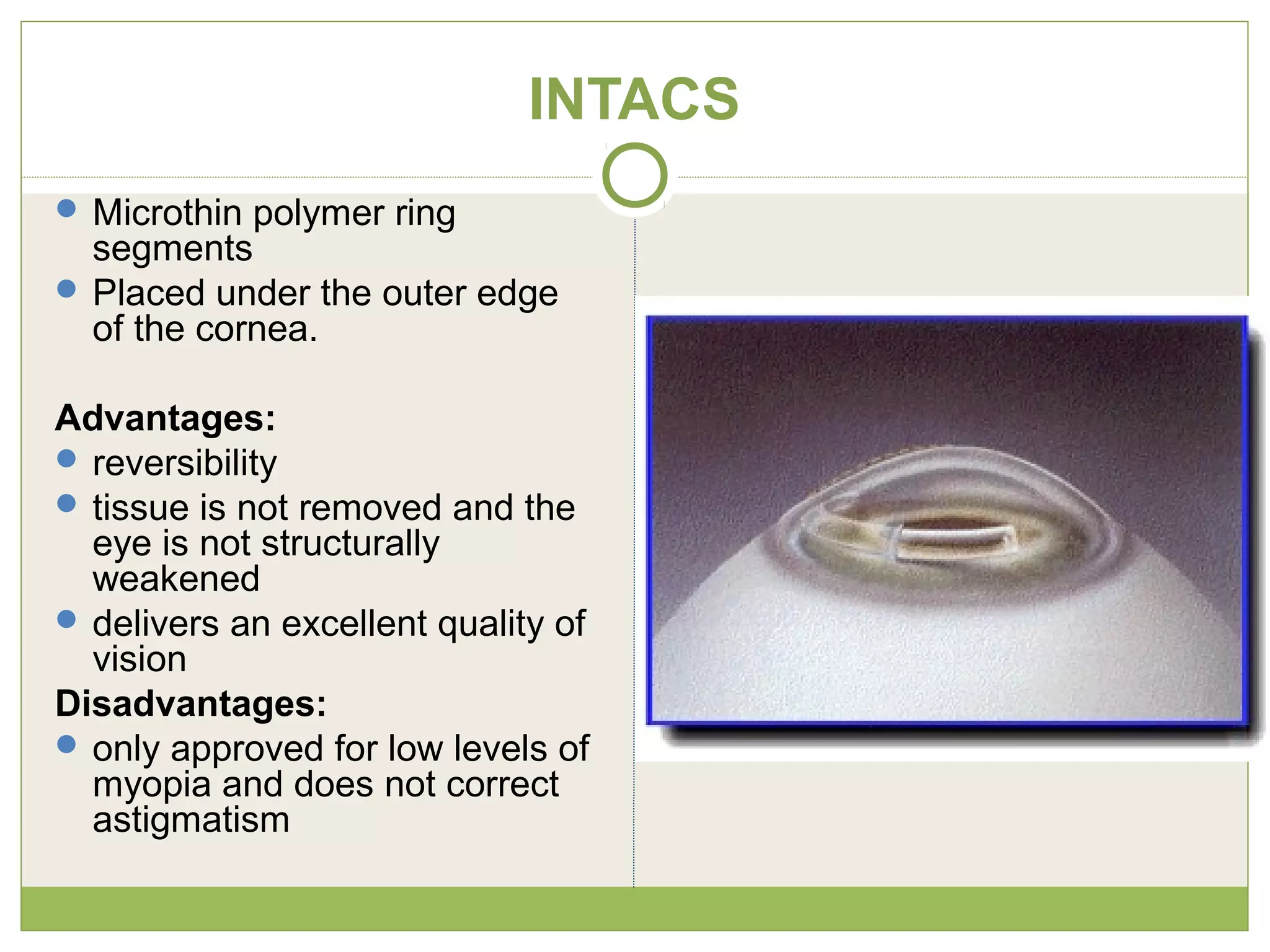
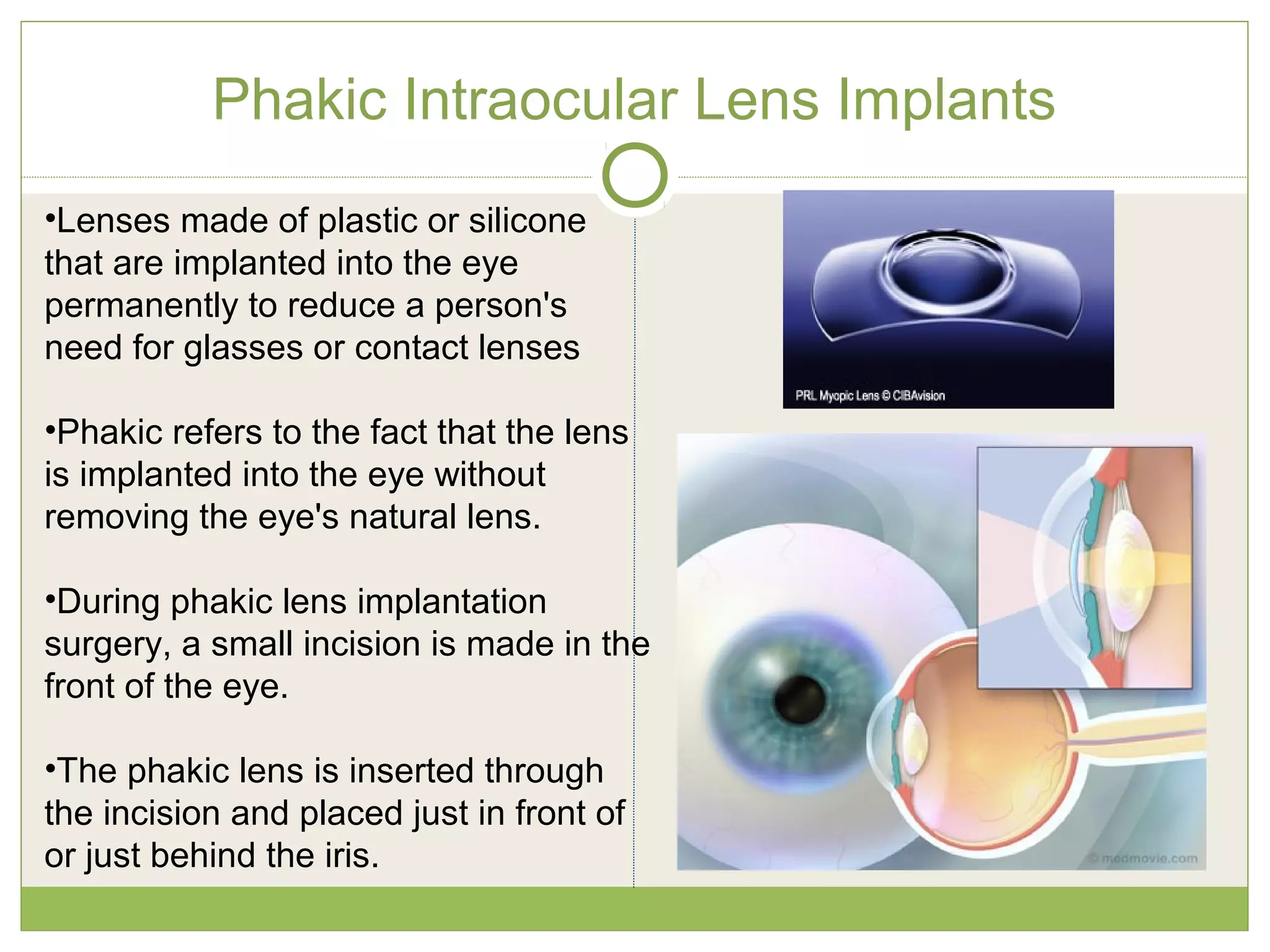


This document provides an overview of refractive errors and their correction presented by Prof. Vijayreddy Vandali. It defines key terms like emmetropia, diopter, and accommodation. It describes different types of refractive errors - hyperopia, myopia, astigmatism, presbyopia and anisometropia. For each error, it discusses causes, signs and symptoms, and methods of correction using lenses, contact lenses or surgery. Surgical procedures discussed for correction include LASIK, PRK, radial keratotomy, INTACS and phakic intraocular lens implants. The document aims to educate about different refractive errors, their diagnosis and management.























































































