Downloaded 88 times





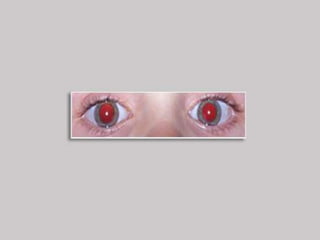



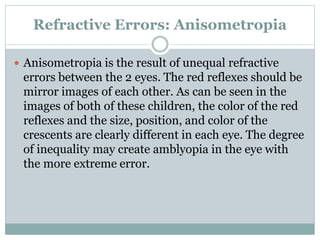

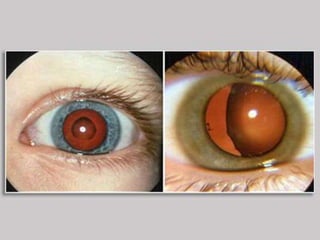

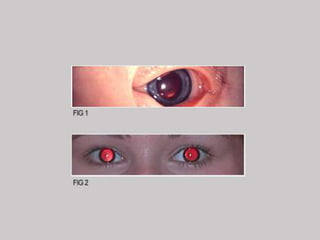






The document outlines the Brückner test, an enhanced vision screening tool for children, requiring only a direct ophthalmoscope and a cooperative child. It screens for common eye disorders such as amblyopia, strabismus, refractive errors, and media opacities through a simple three-step procedure involving assessment of the red reflex. The test not only identifies refractive errors like hyperopia and myopia but also detects serious conditions like cataracts and retinoblastoma.















































































