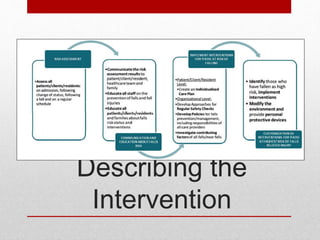
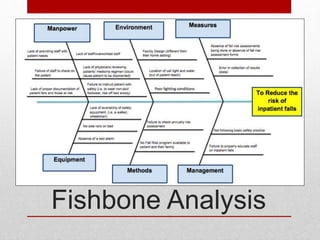
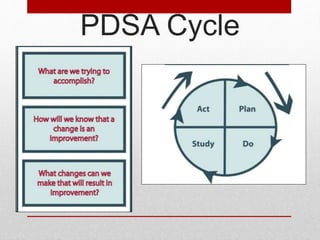
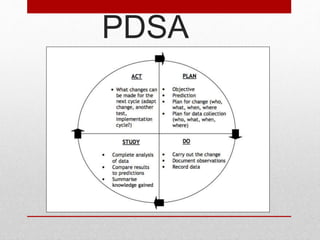
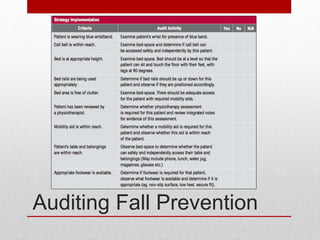
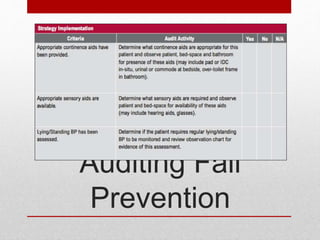
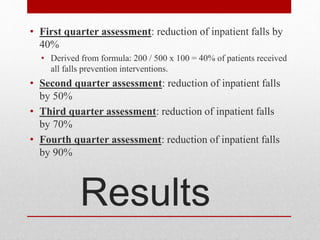
The document outlines a quality improvement initiative at Sun Coast Regional Hospital to reduce their inpatient fall rate of 50% per 1,000 patients annually. The team aims to reduce the rate by 90% through interventions targeting materials (patient/staff education), physical environment (facility design), and workforce (increasing staffing). They conduct a fishbone analysis, implement interventions using the PDSA model, measure quarterly results, and continue refining interventions such as enforcing footwear/wristband rules and routine physiotherapy checks.