Downloaded 24 times
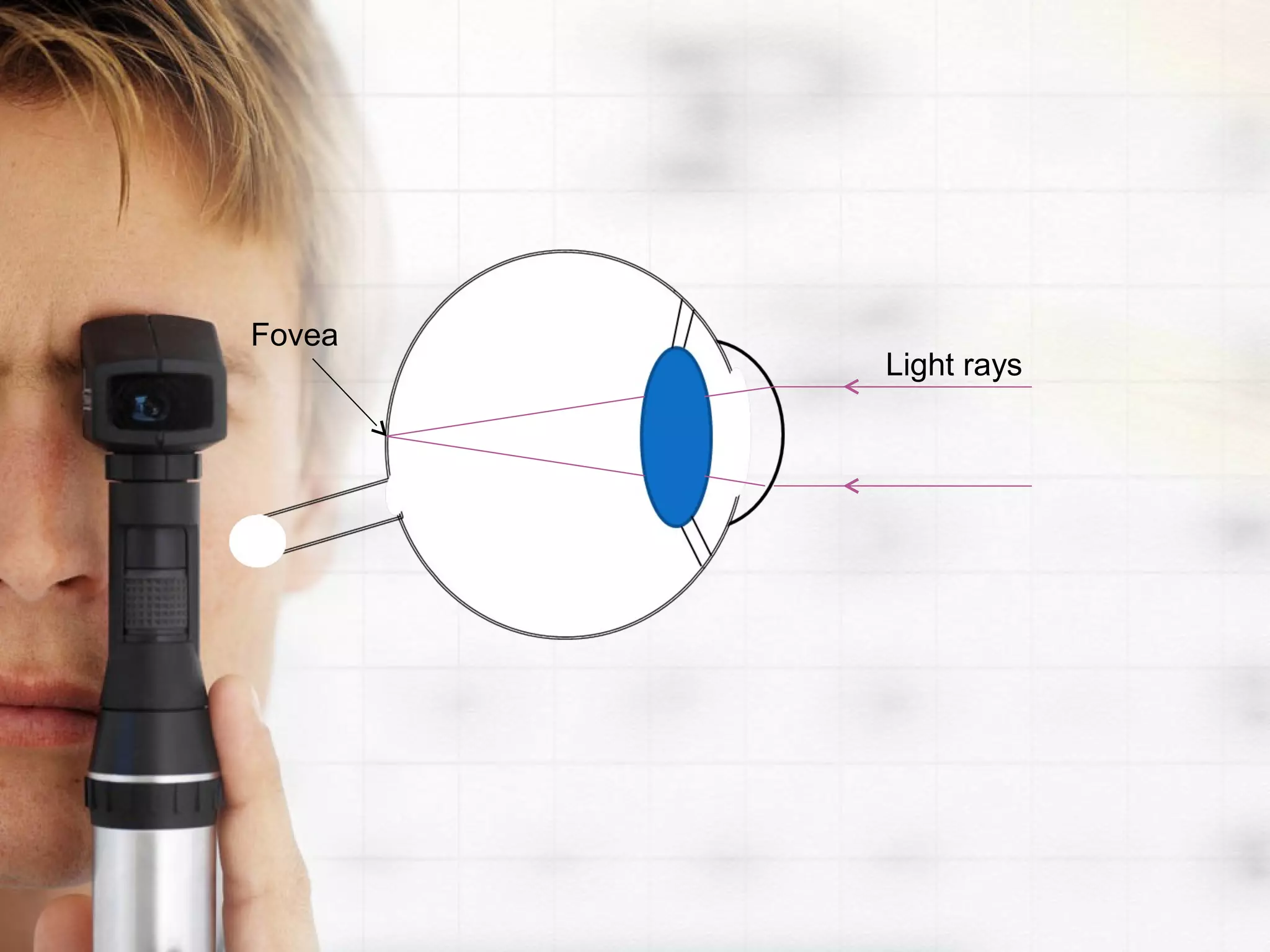
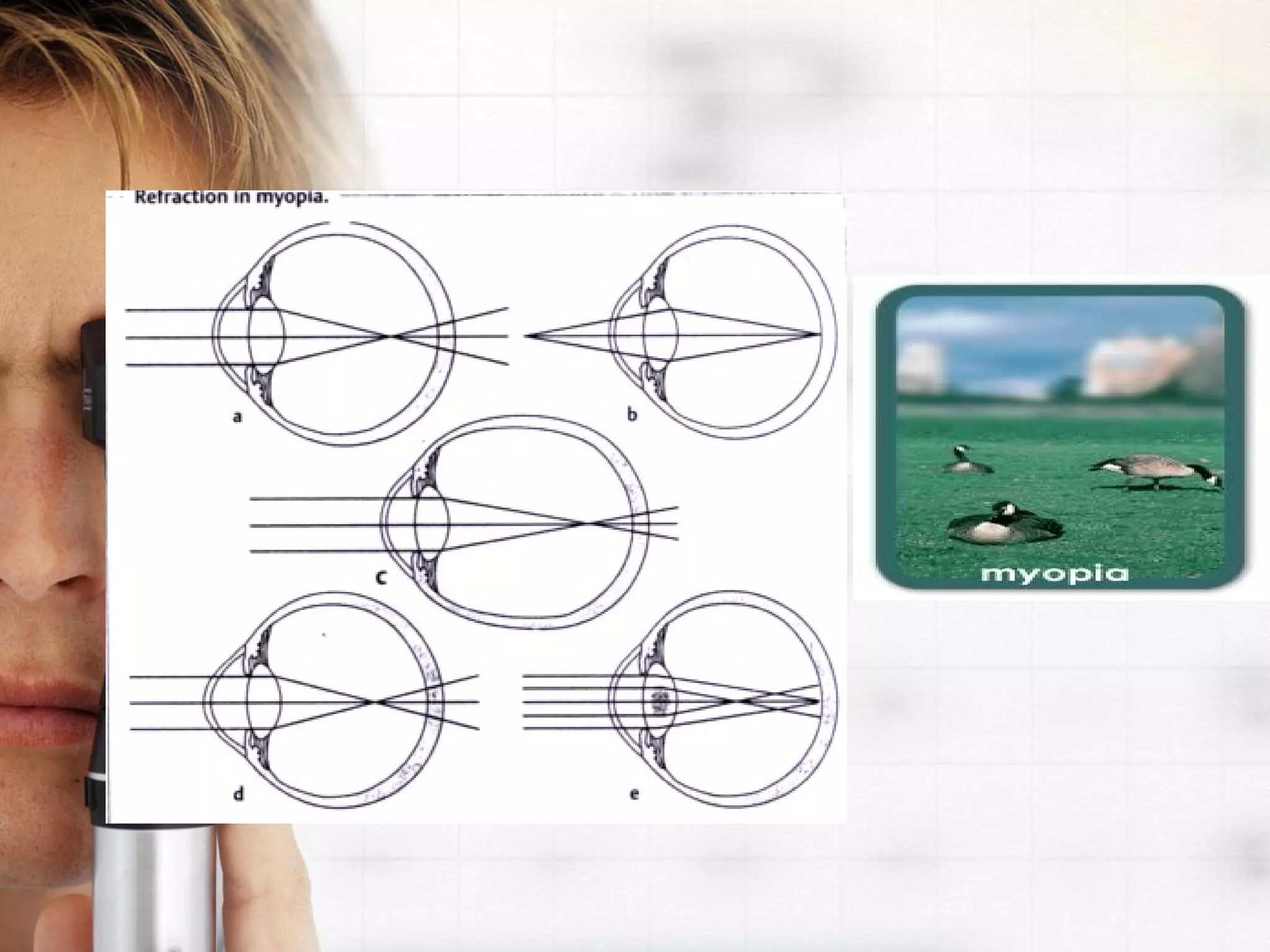
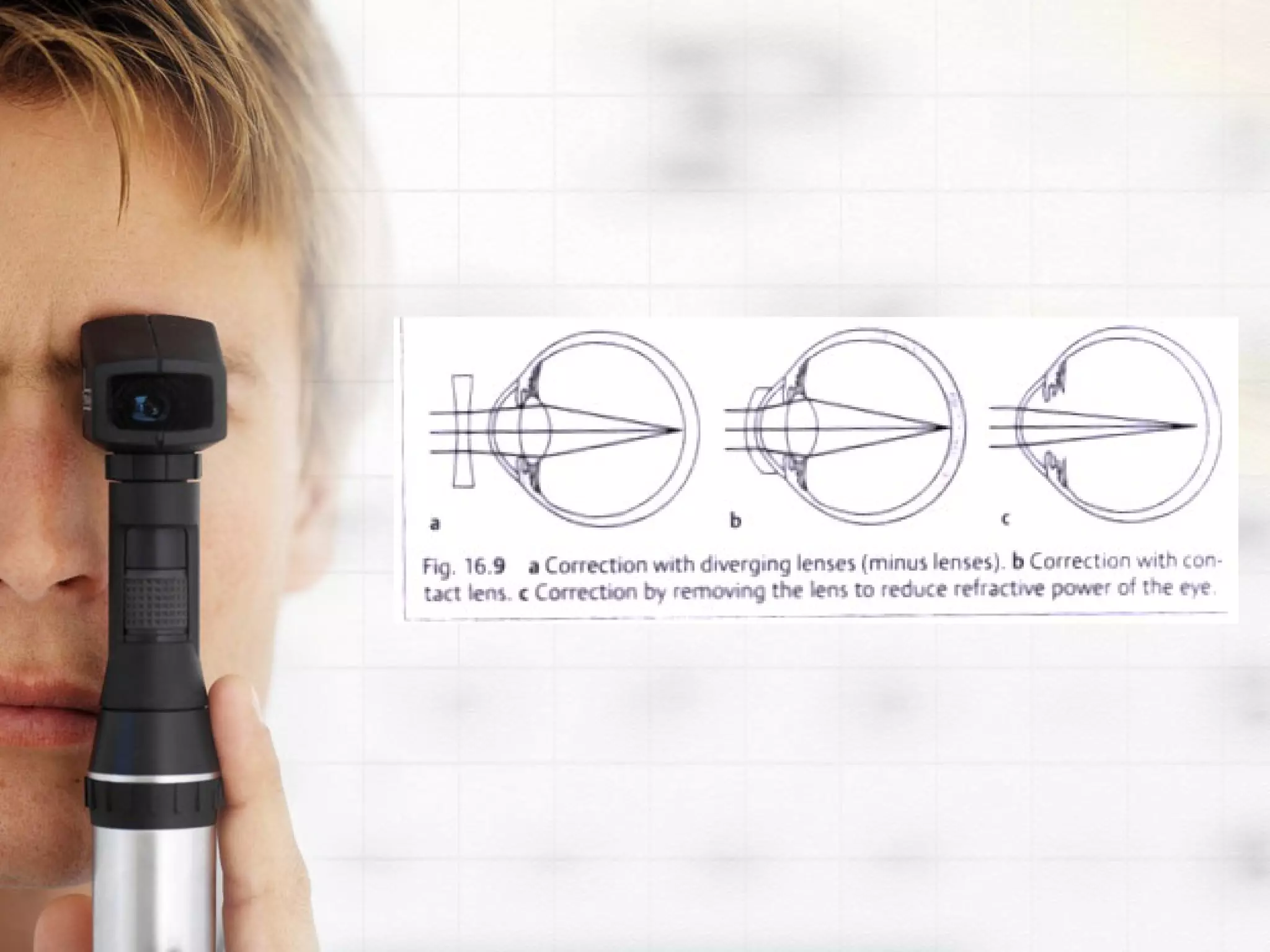
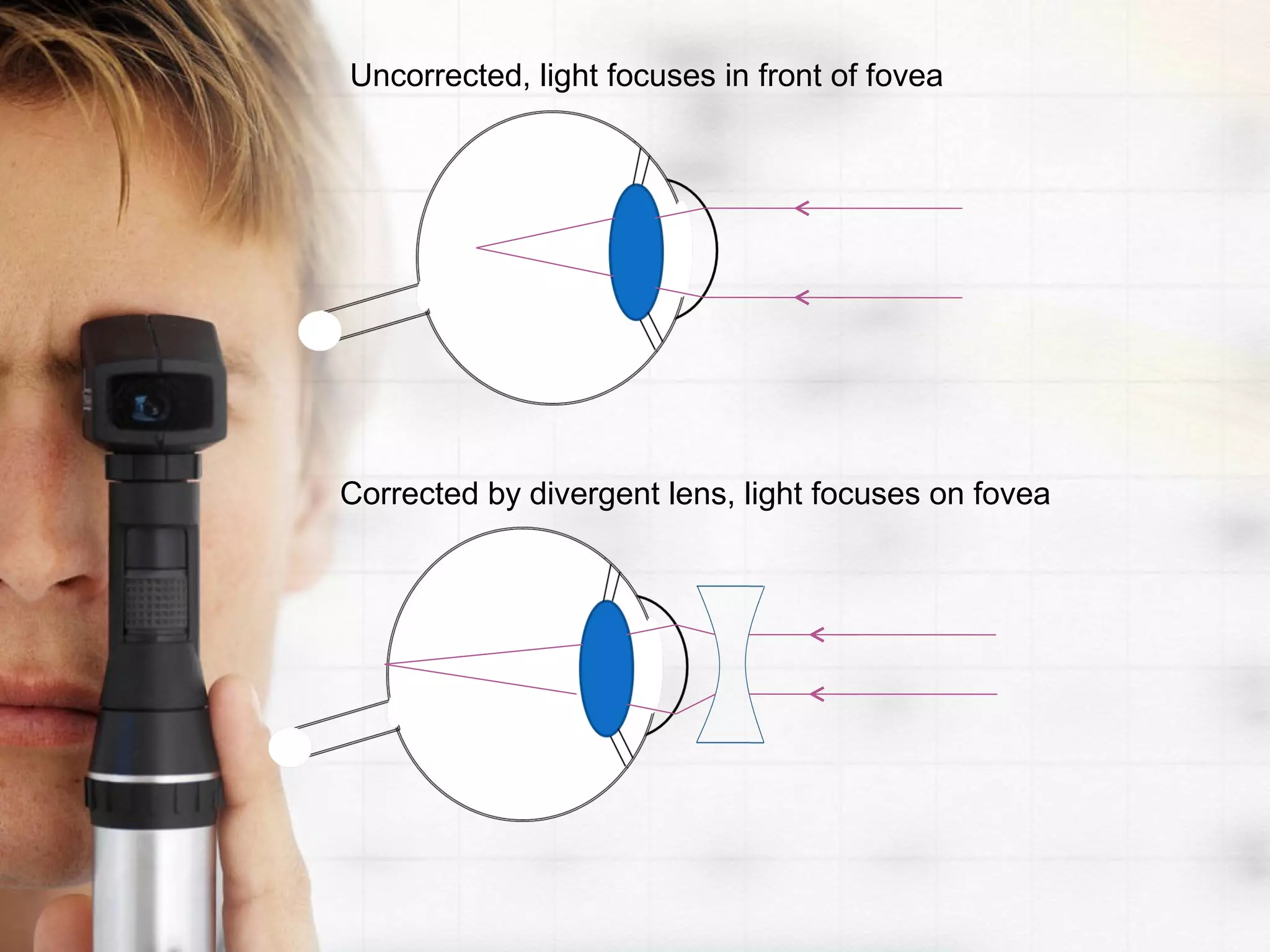
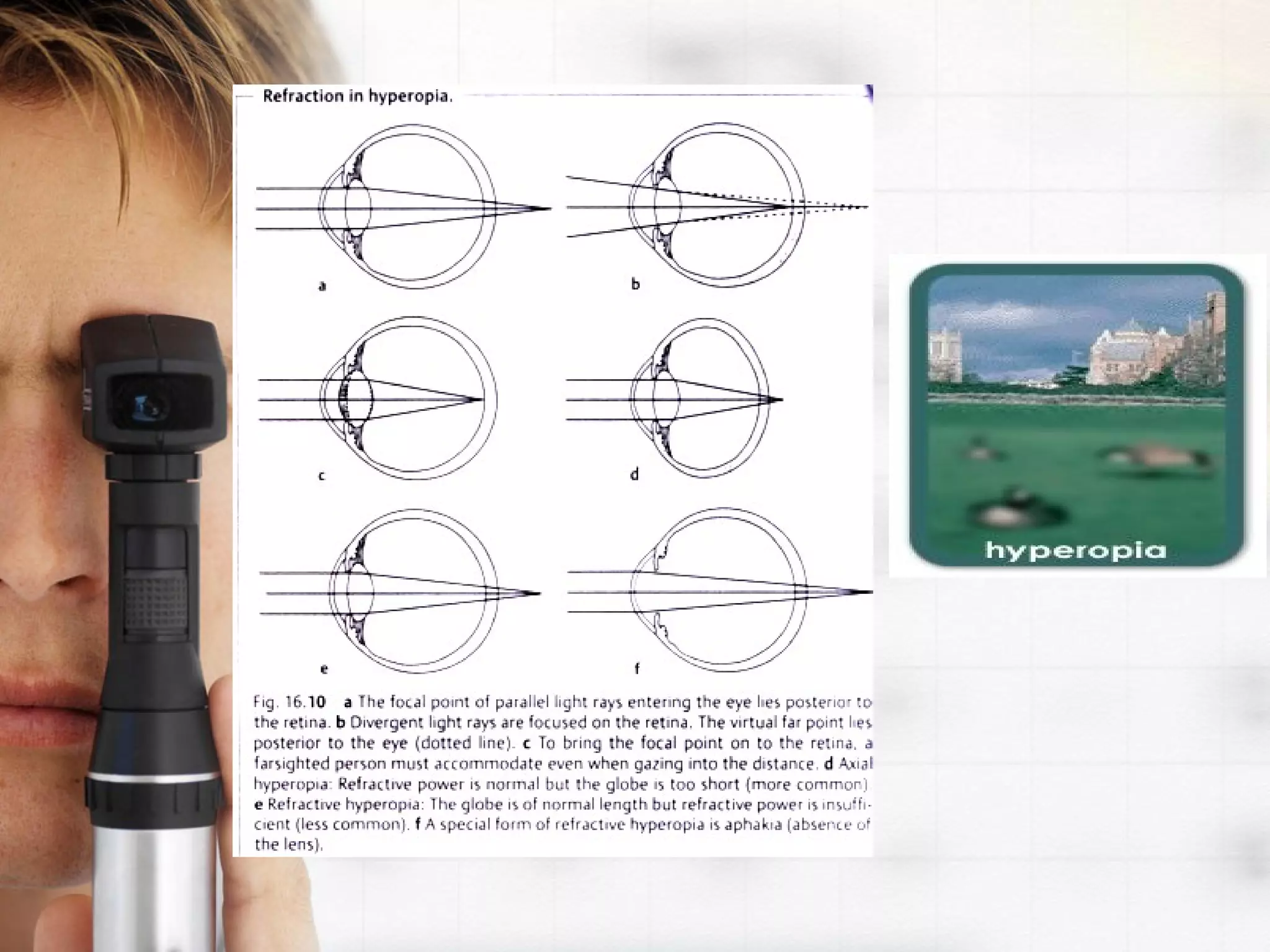
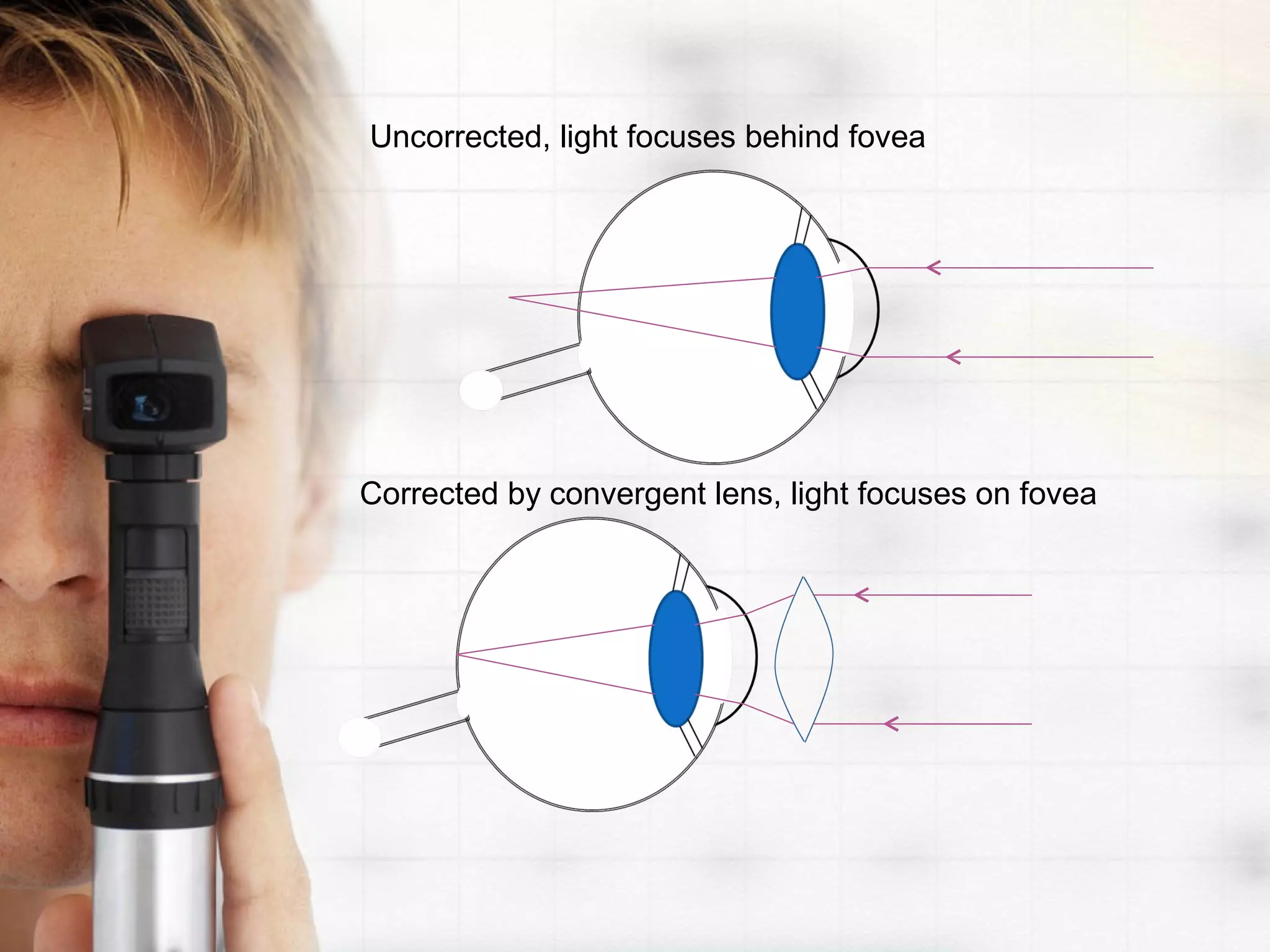
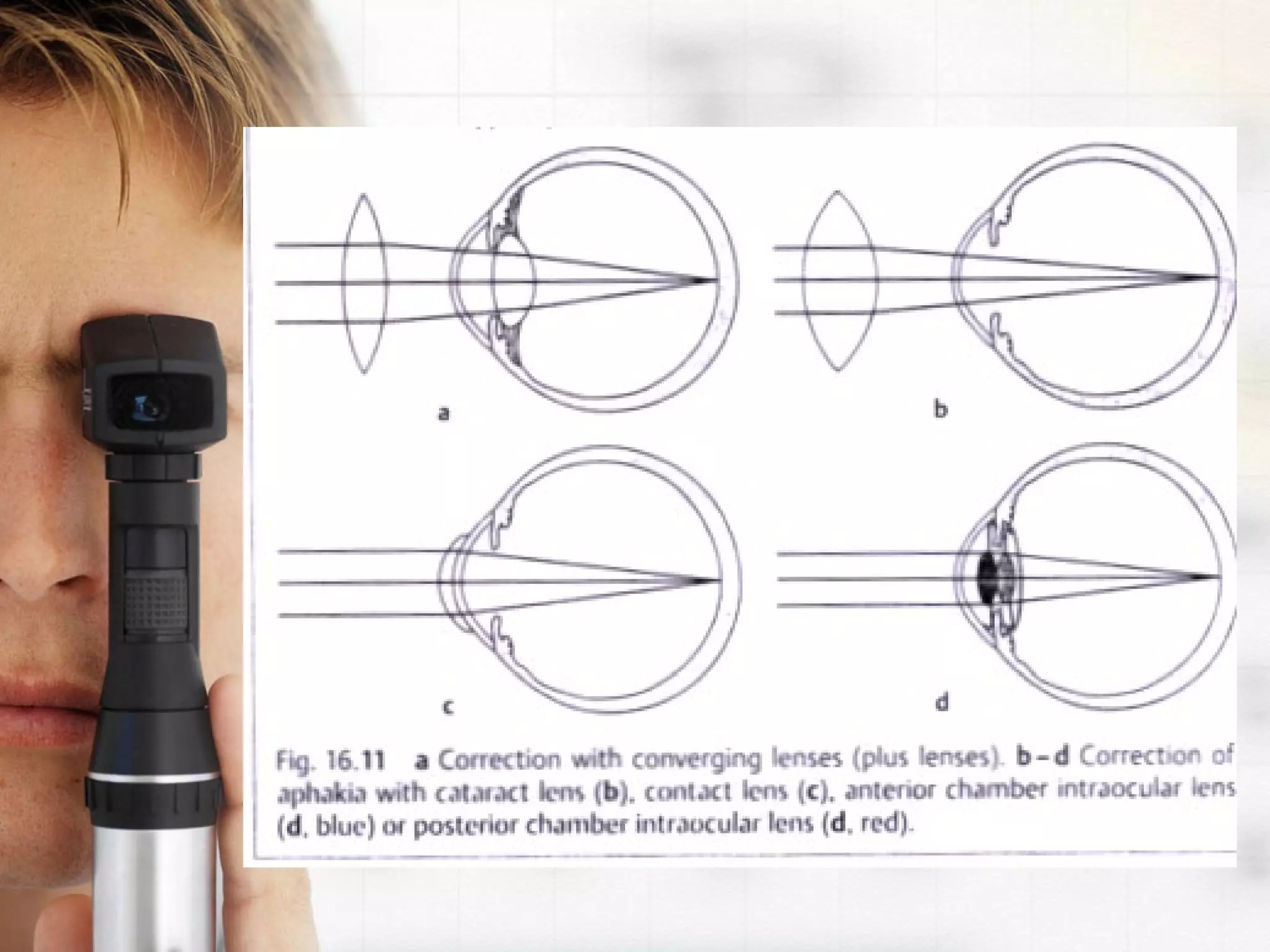
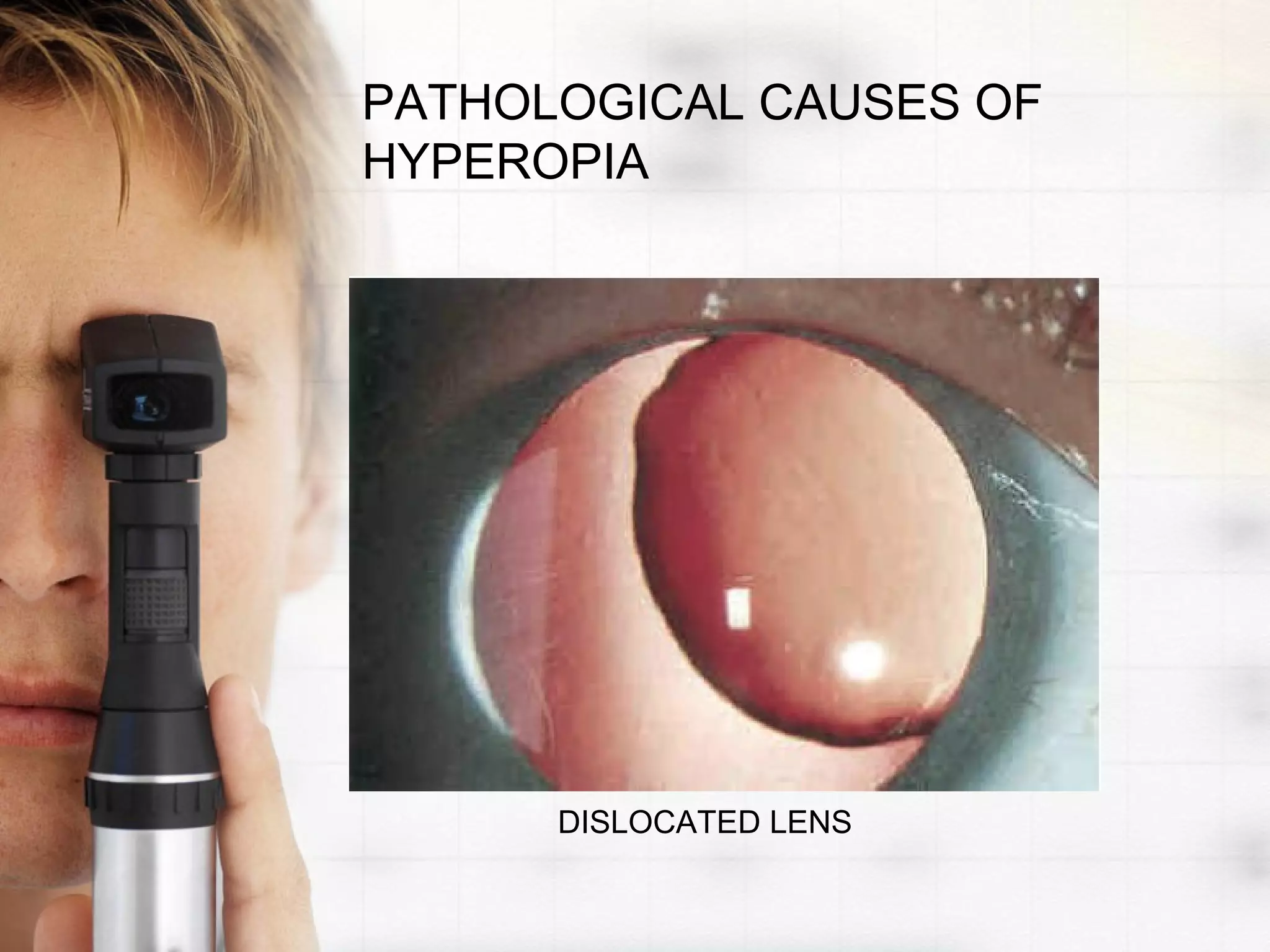
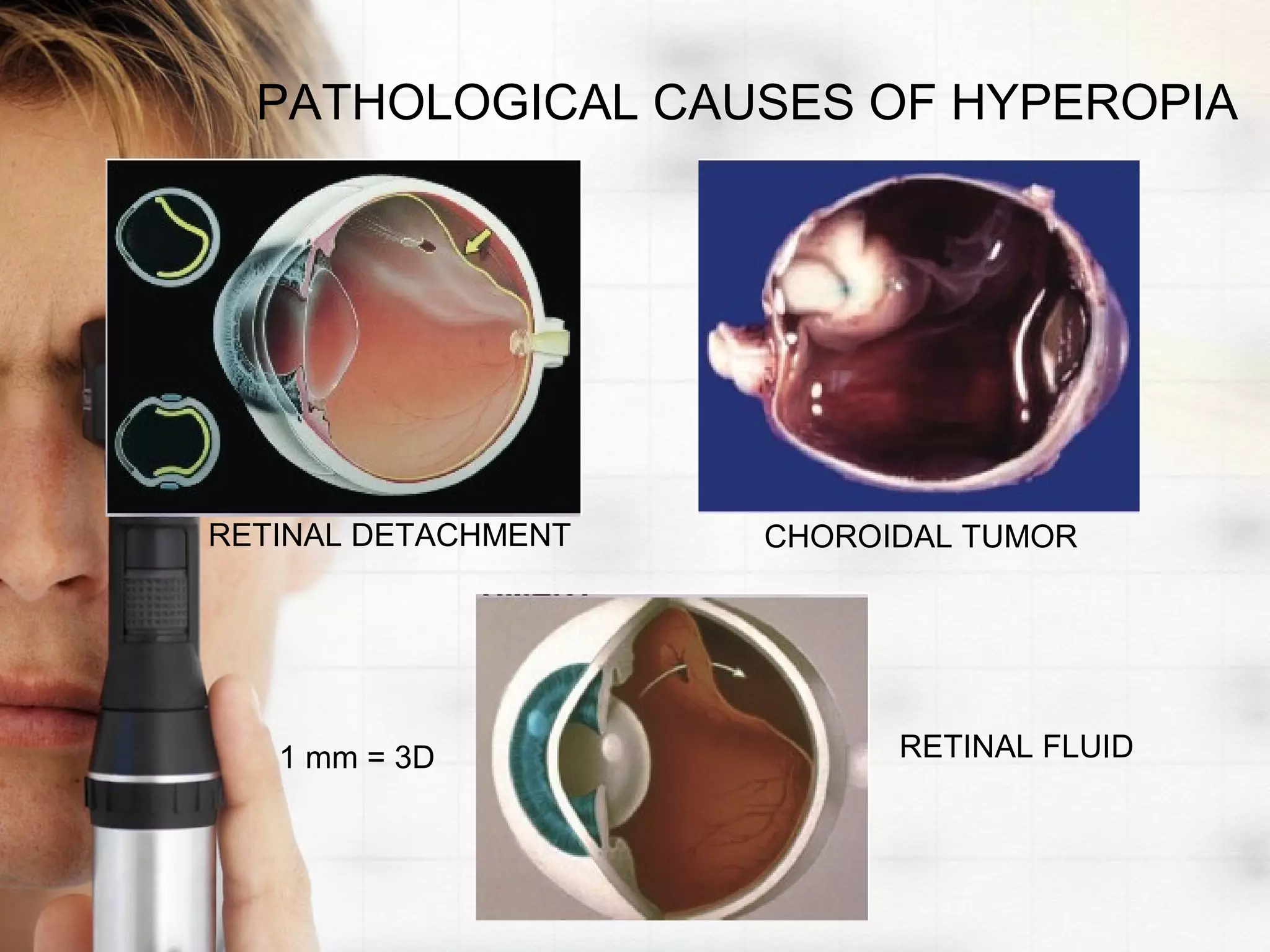
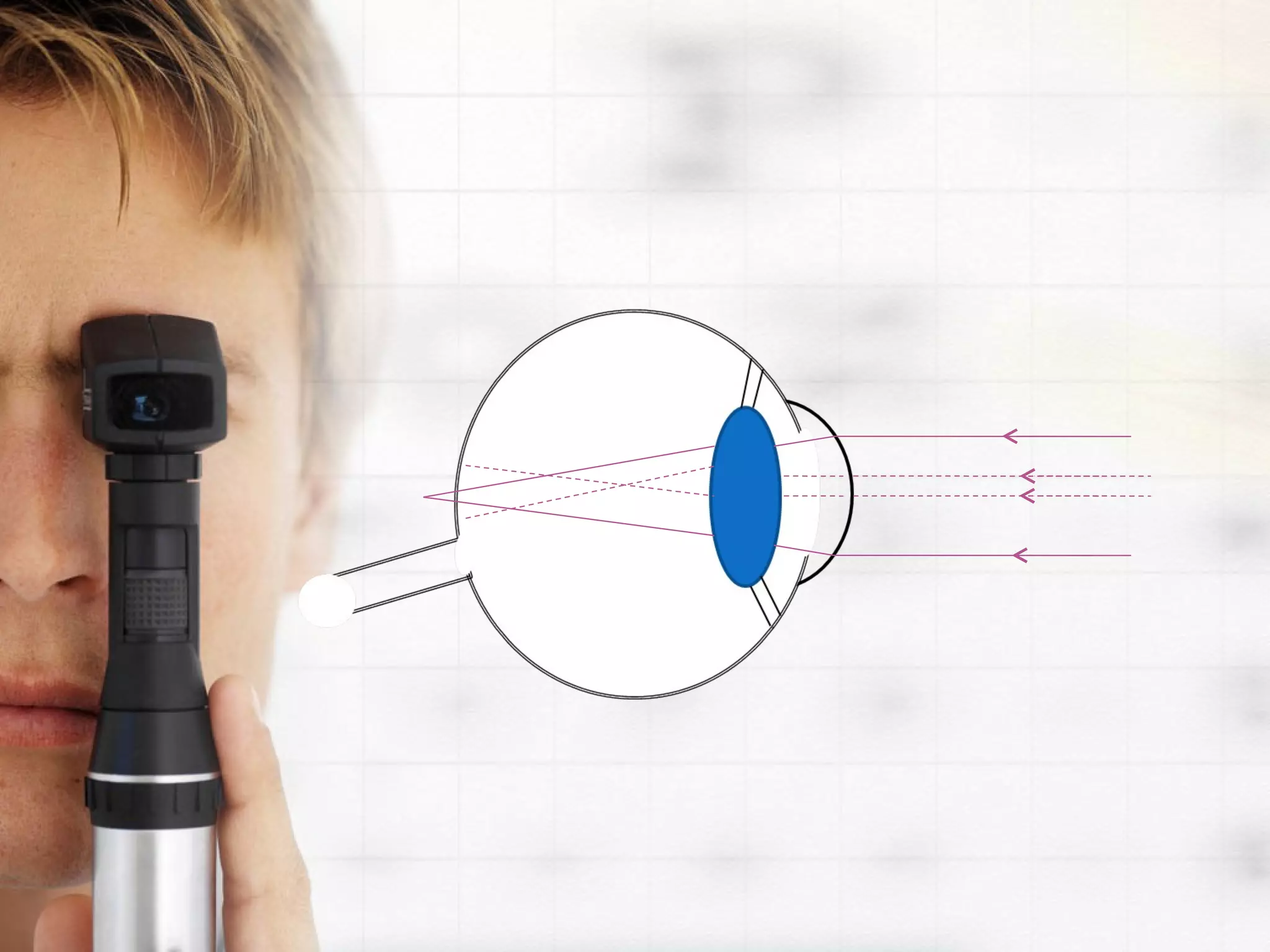

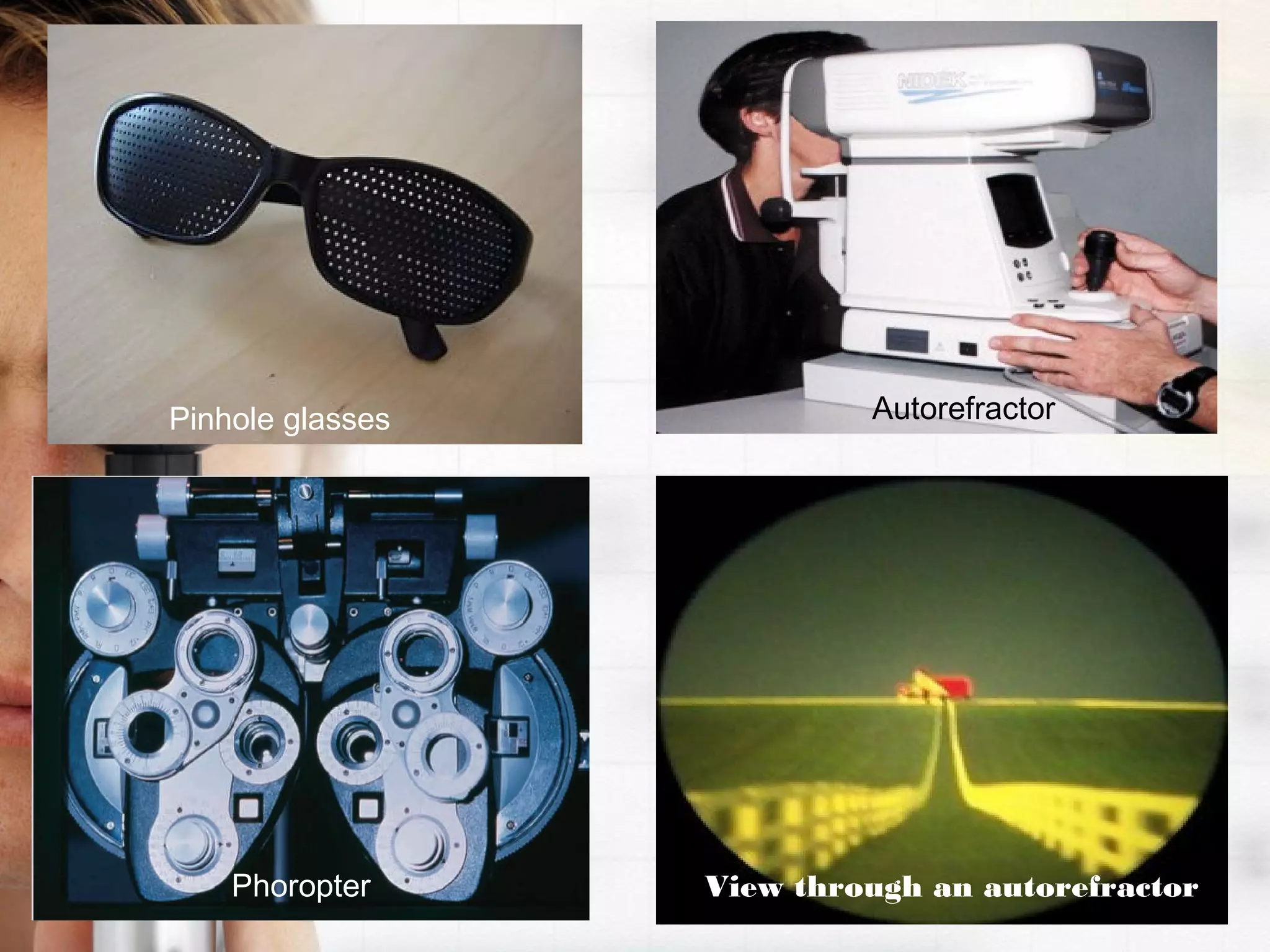

Refractive errors occur when there is a mismatch between the eye's optical power and its axial length. The most common refractive errors are myopia, hyperopia, and astigmatism. Myopia occurs when the eye's axial length is too long, causing light to focus in front of the retina. Hyperopia is the opposite, with light focusing behind the retina due to a shorter axial length. Astigmatism causes blurred vision due to an irregularly shaped cornea or lens. These refractive errors can be corrected using glasses, contact lenses, refractive surgery, or intraocular lenses. A complete eye exam using tools like a phoropter and autorefractor can diagnose a patient's refractive error.























































































