
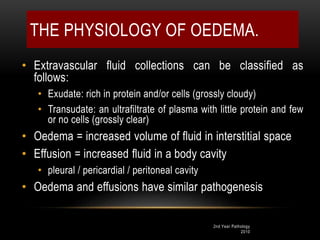
![Oedema fluid may be:
• 1] transudate which is more often the case, such as in oedema
of cardiac and renal disease; or
• 2] exudate such as in inflammatory oedema.
The differences between transudate and exudate are tabulated.](https://image.slidesharecdn.com/patofisiologiedemafkunismuh-200315170439/85/Patofisiologi-edema-32-320.jpg)
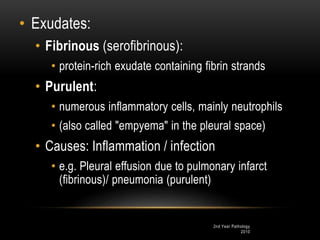

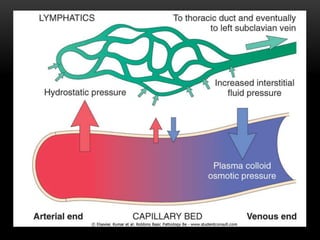
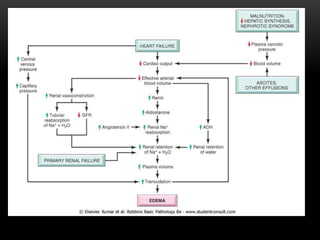
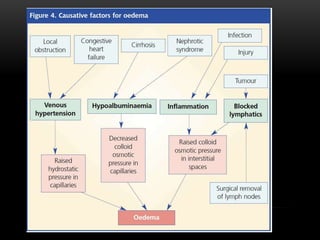

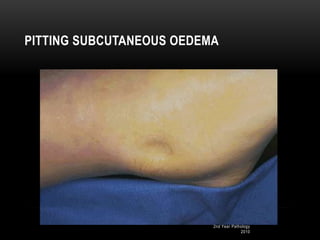
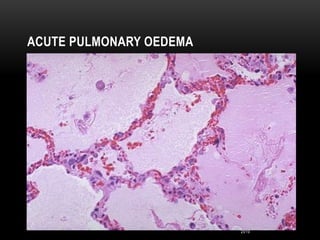



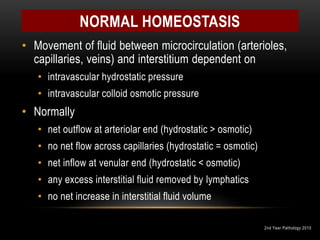
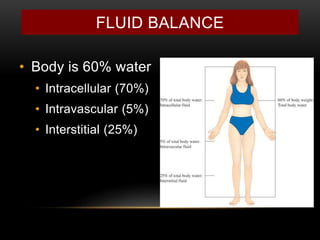
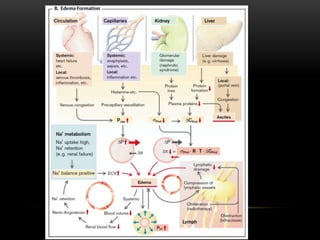
Oedema, or swelling, is caused by an abnormal accumulation of fluid in the interstitial tissue spaces. There are two main types - localized oedema affecting an organ or limb, and generalized oedema known as anasarca. The physiology of oedema involves a balance between hydrostatic pressure pushing fluid out of blood vessels and oncotic pressure pulling fluid back in. Disruptions to this balance that can cause oedema include decreased oncotic pressure, increased hydrostatic pressure, lymphatic obstruction, and increased capillary permeability. Common causes of oedema include cardiac, renal, and hepatic diseases.


































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

















