Downloaded 946 times


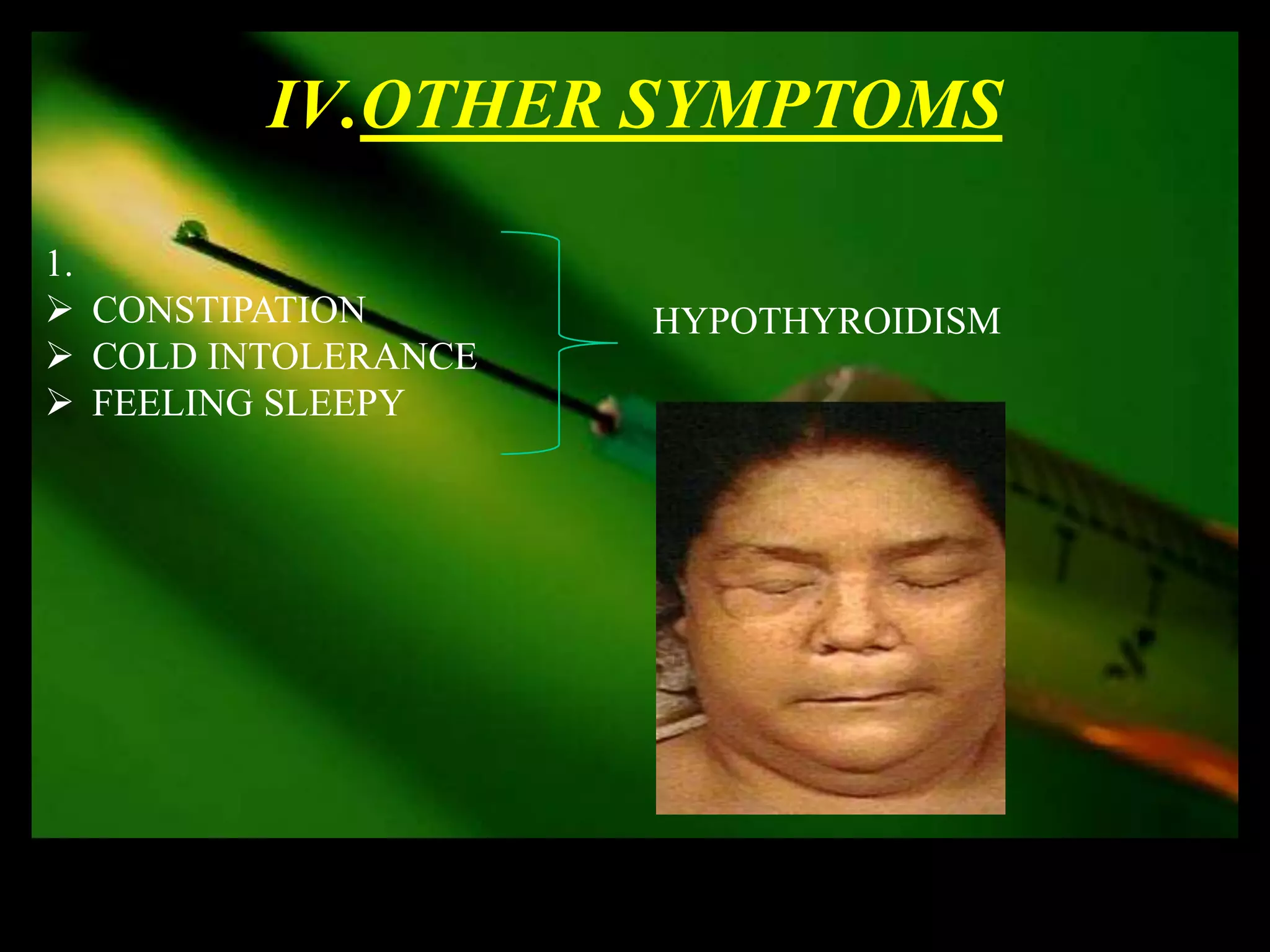
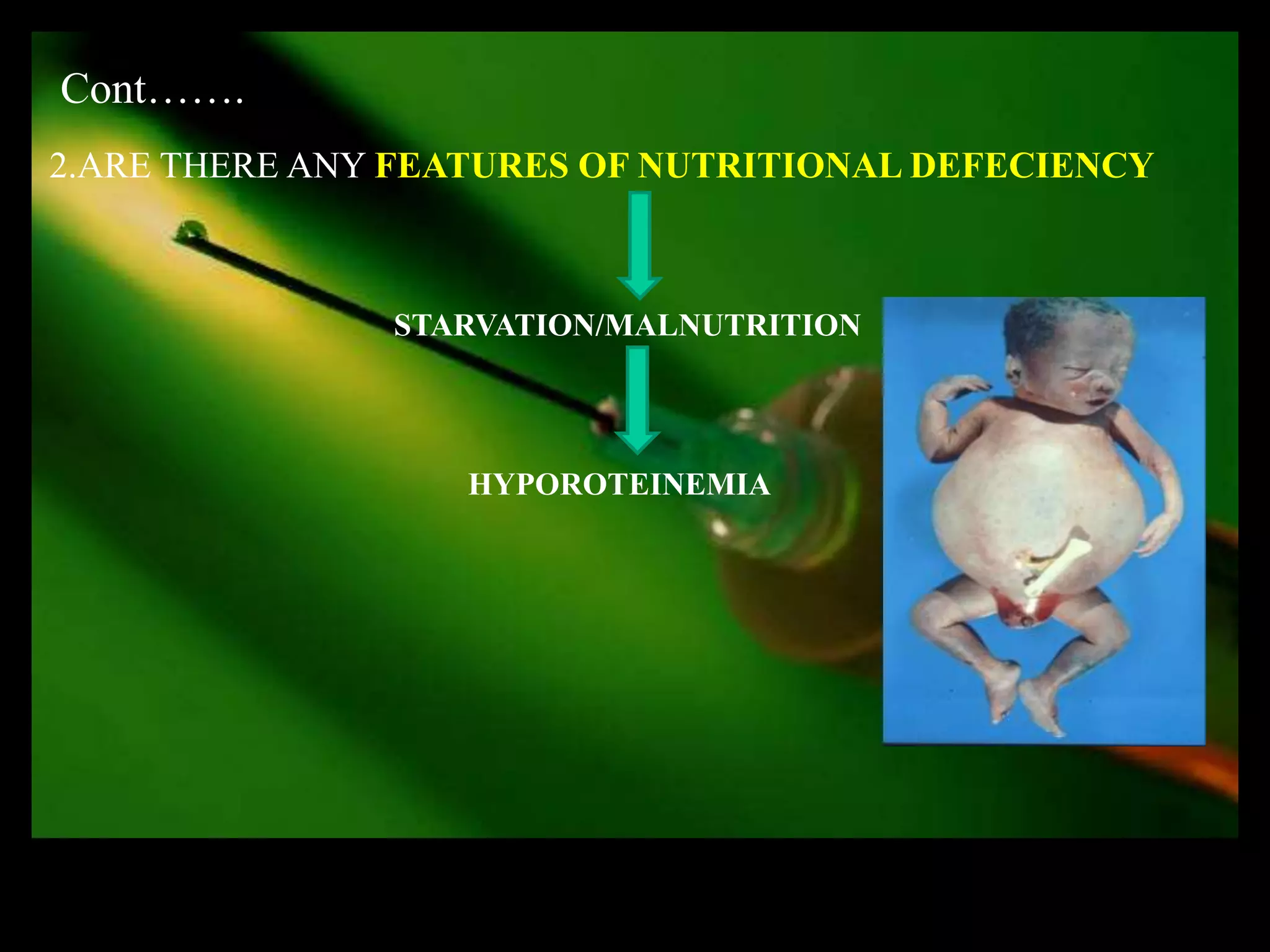
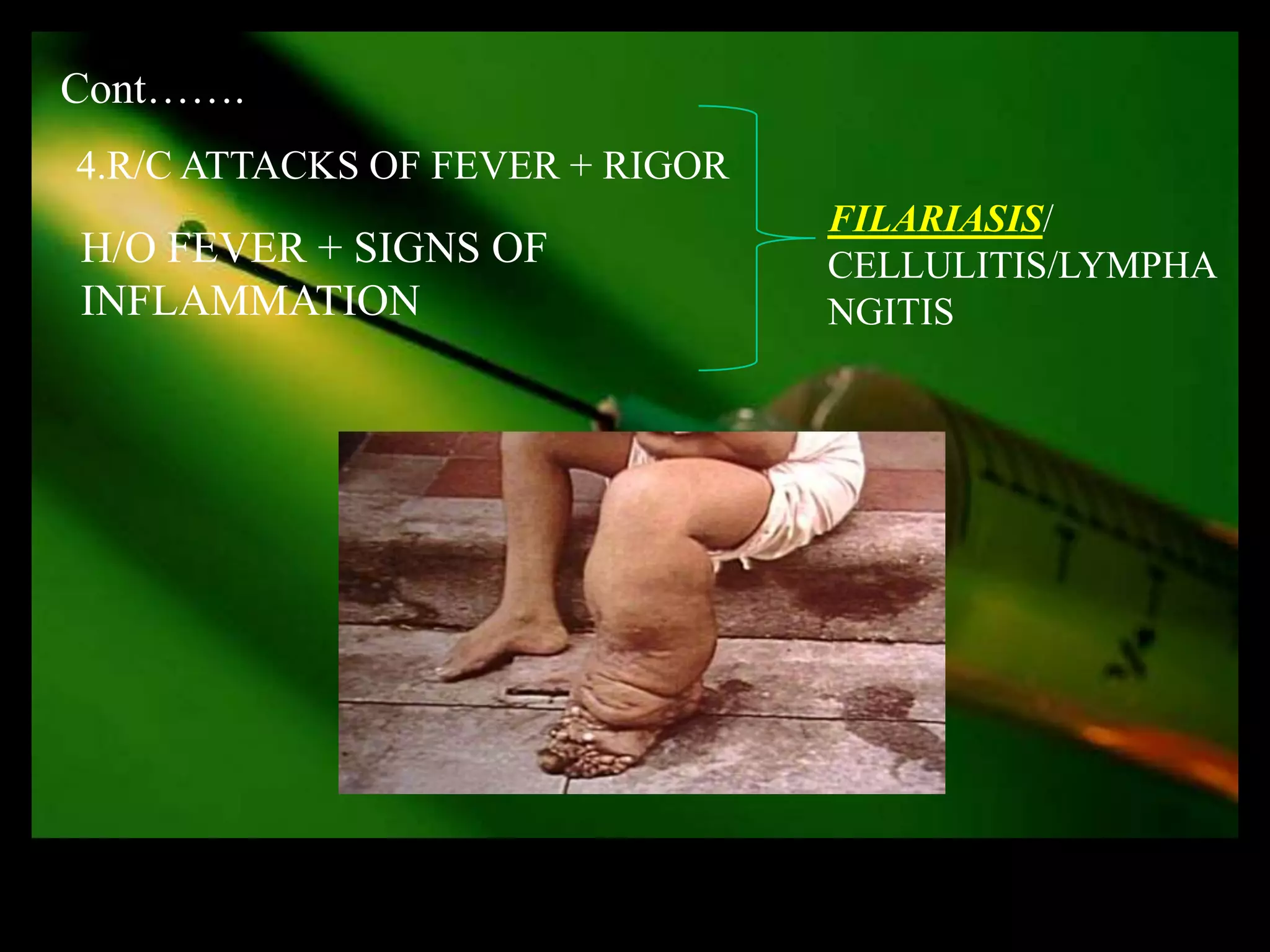
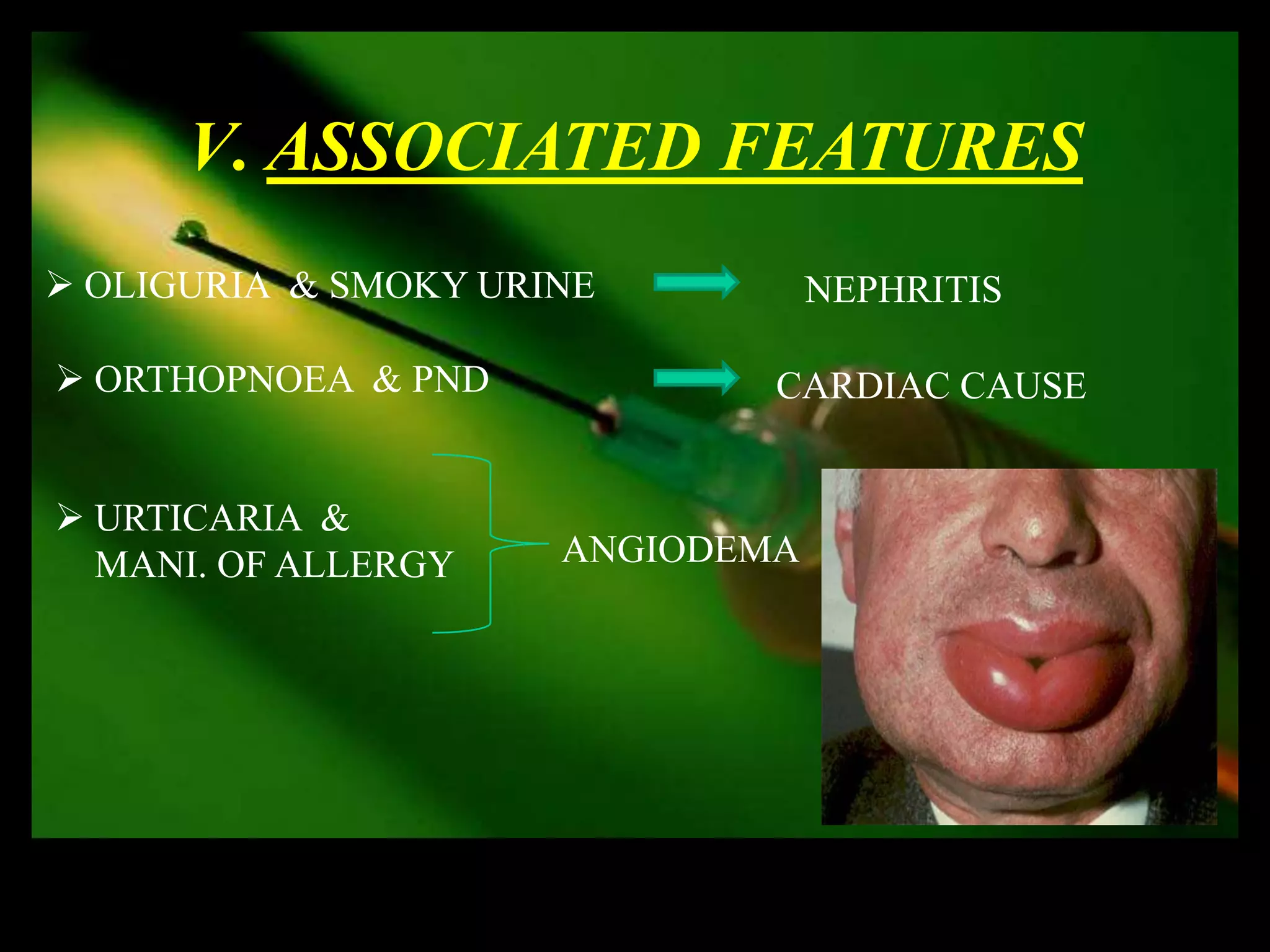


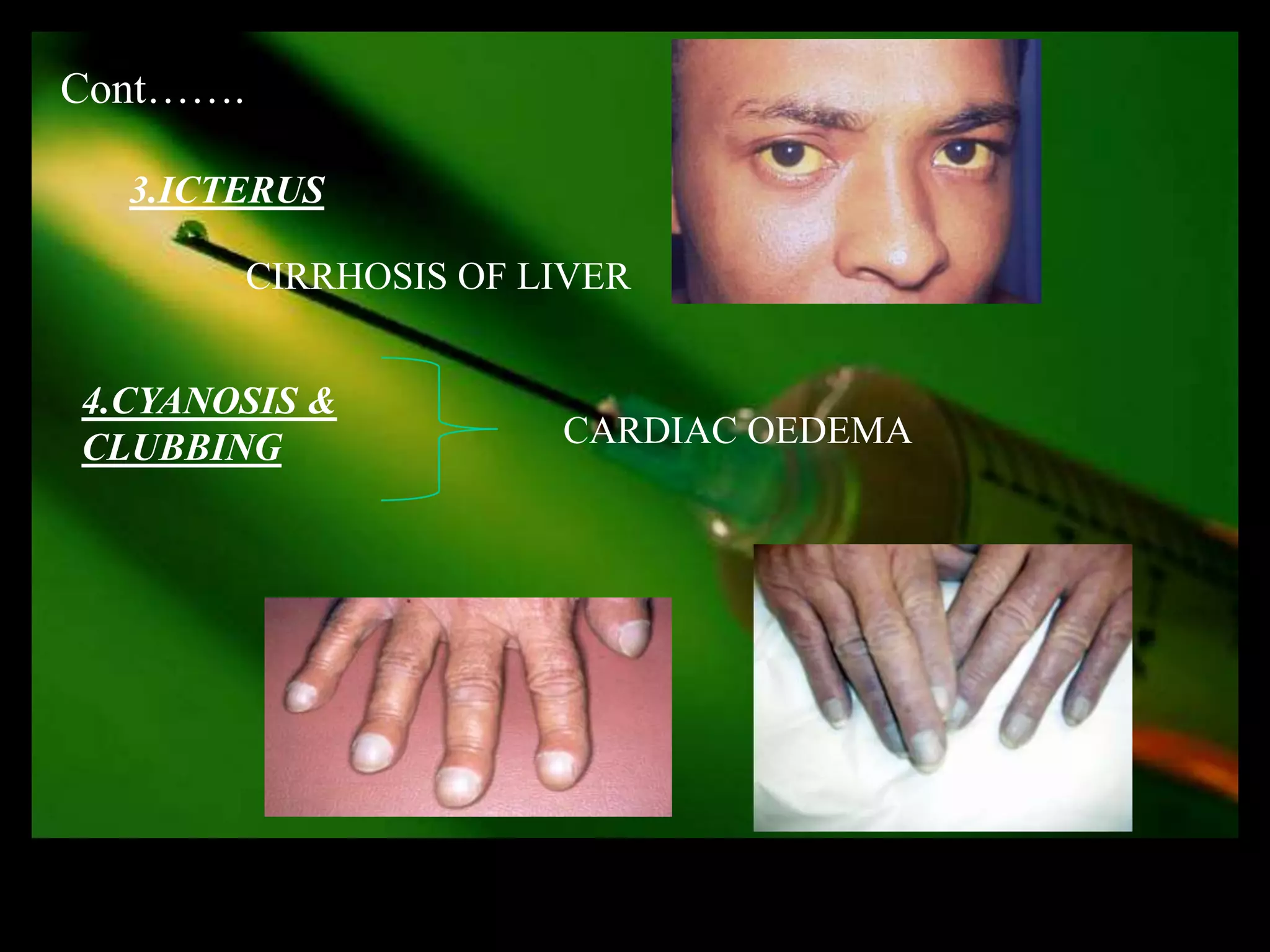
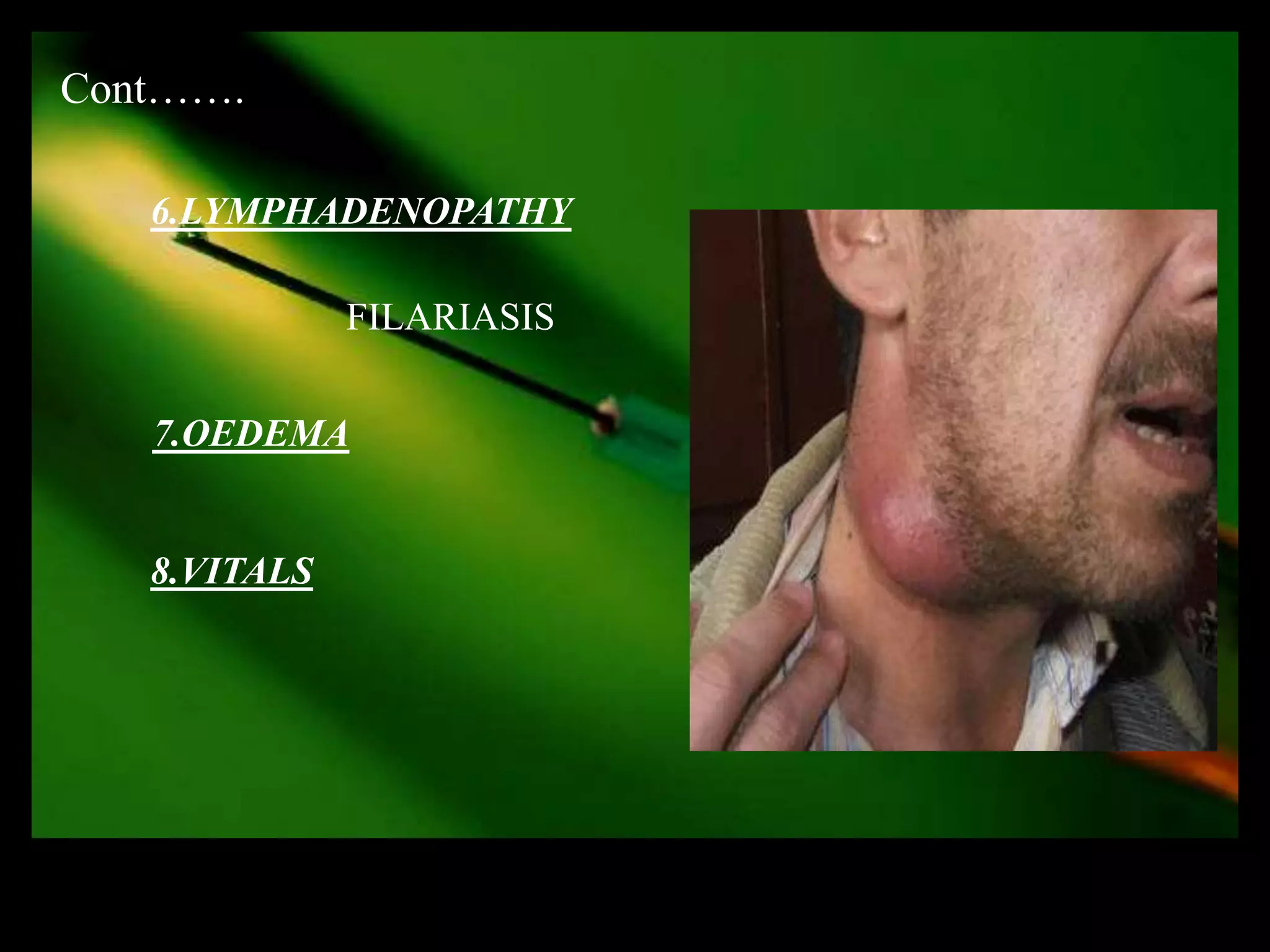
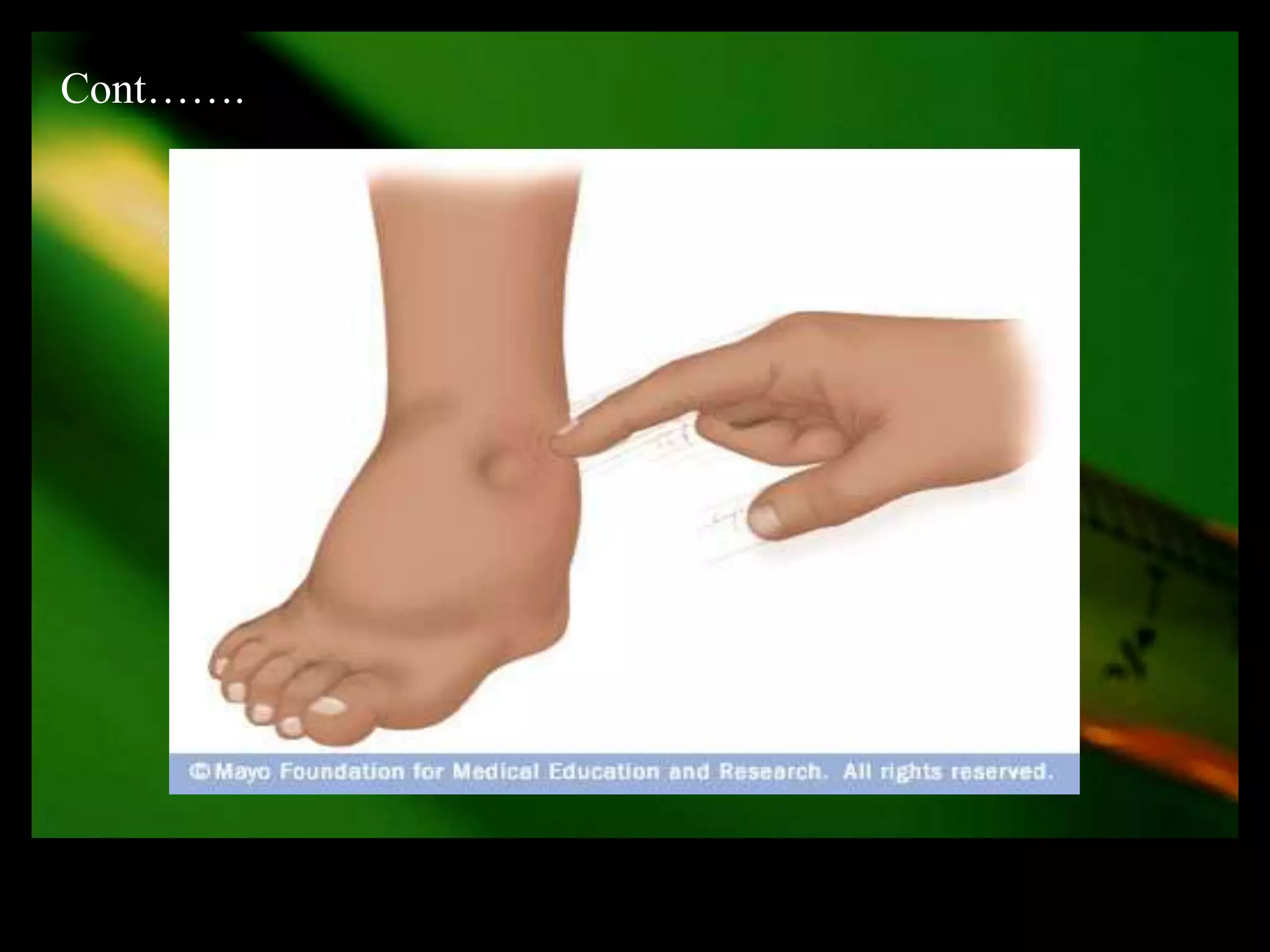
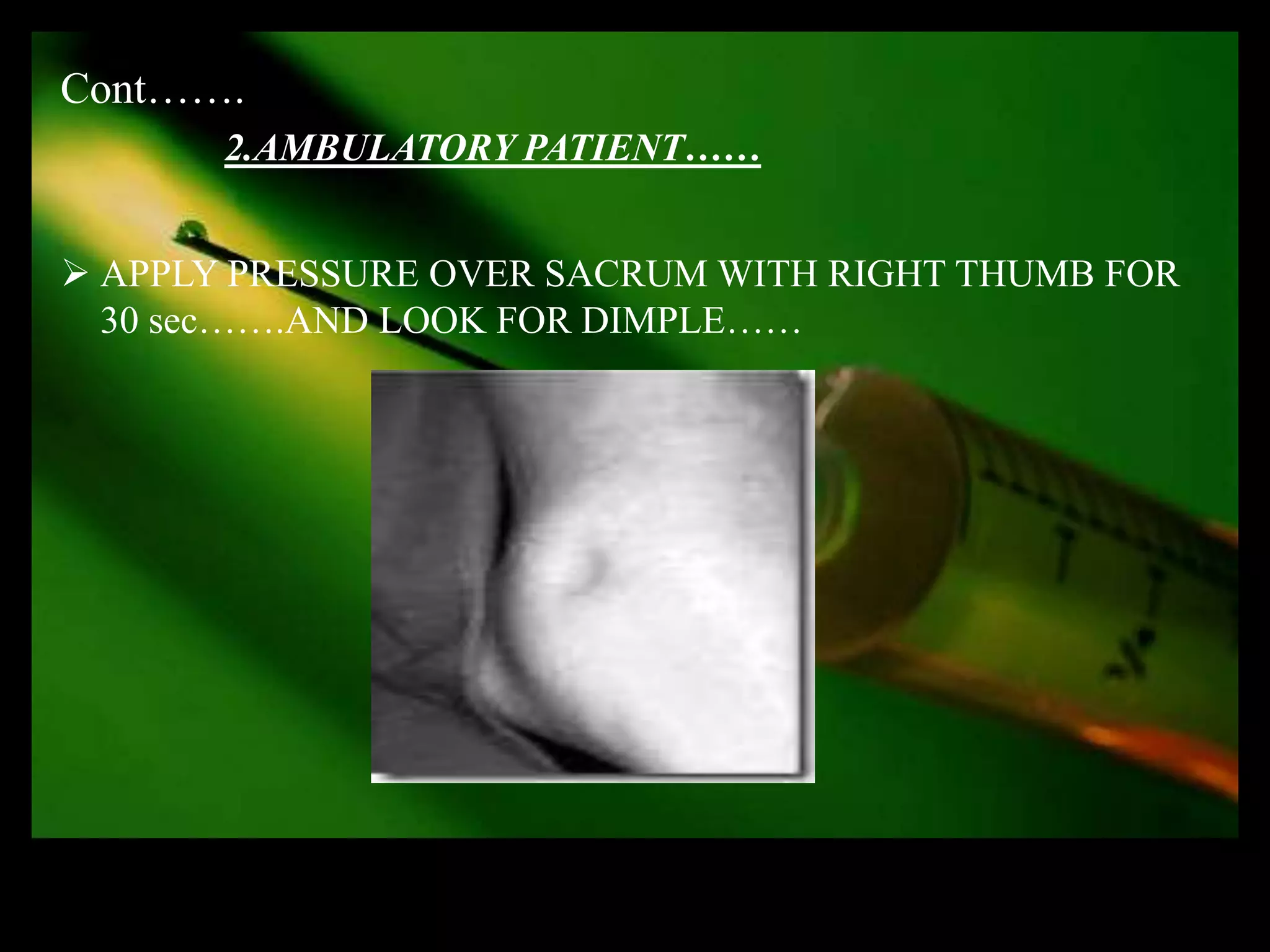
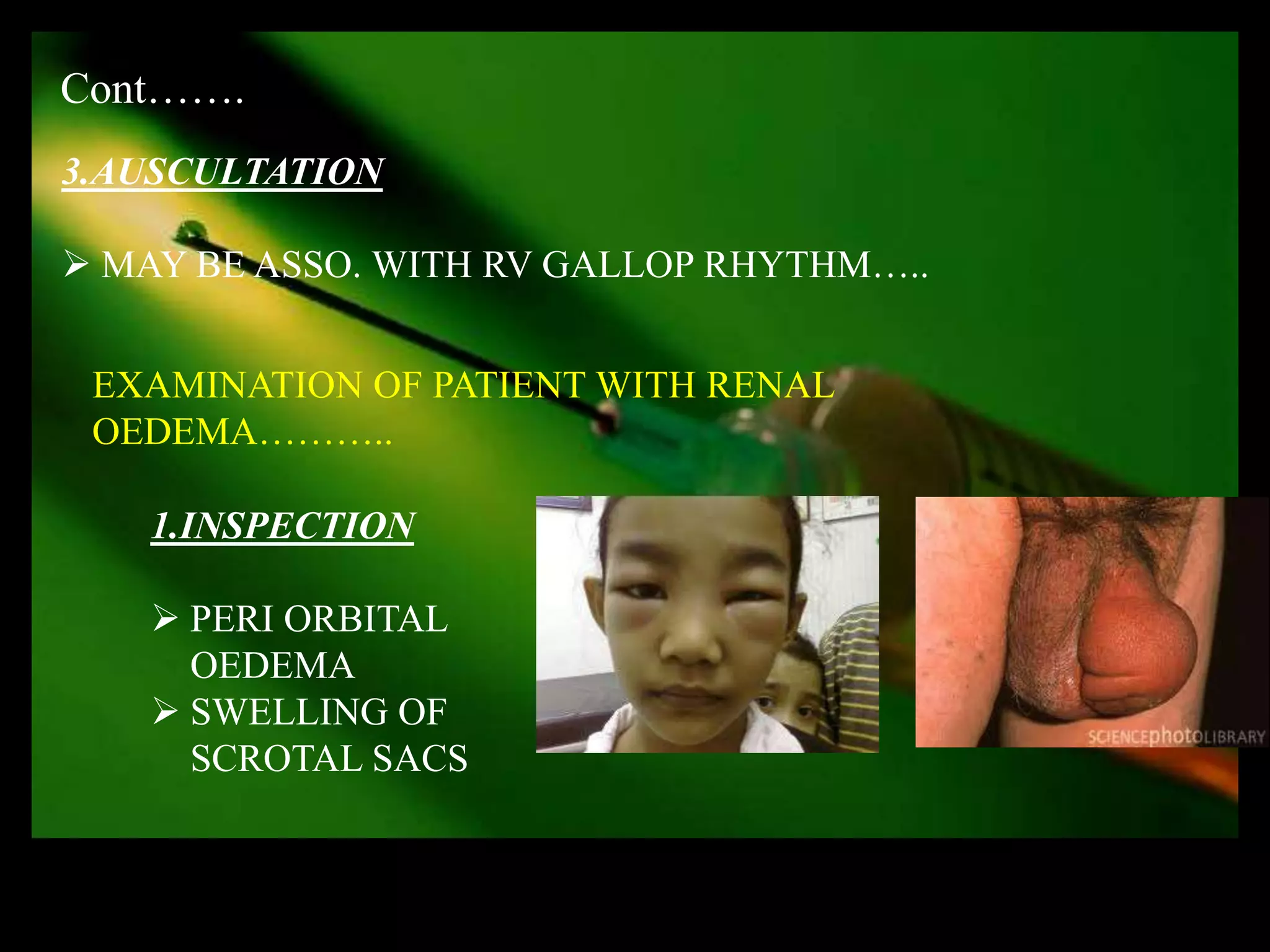
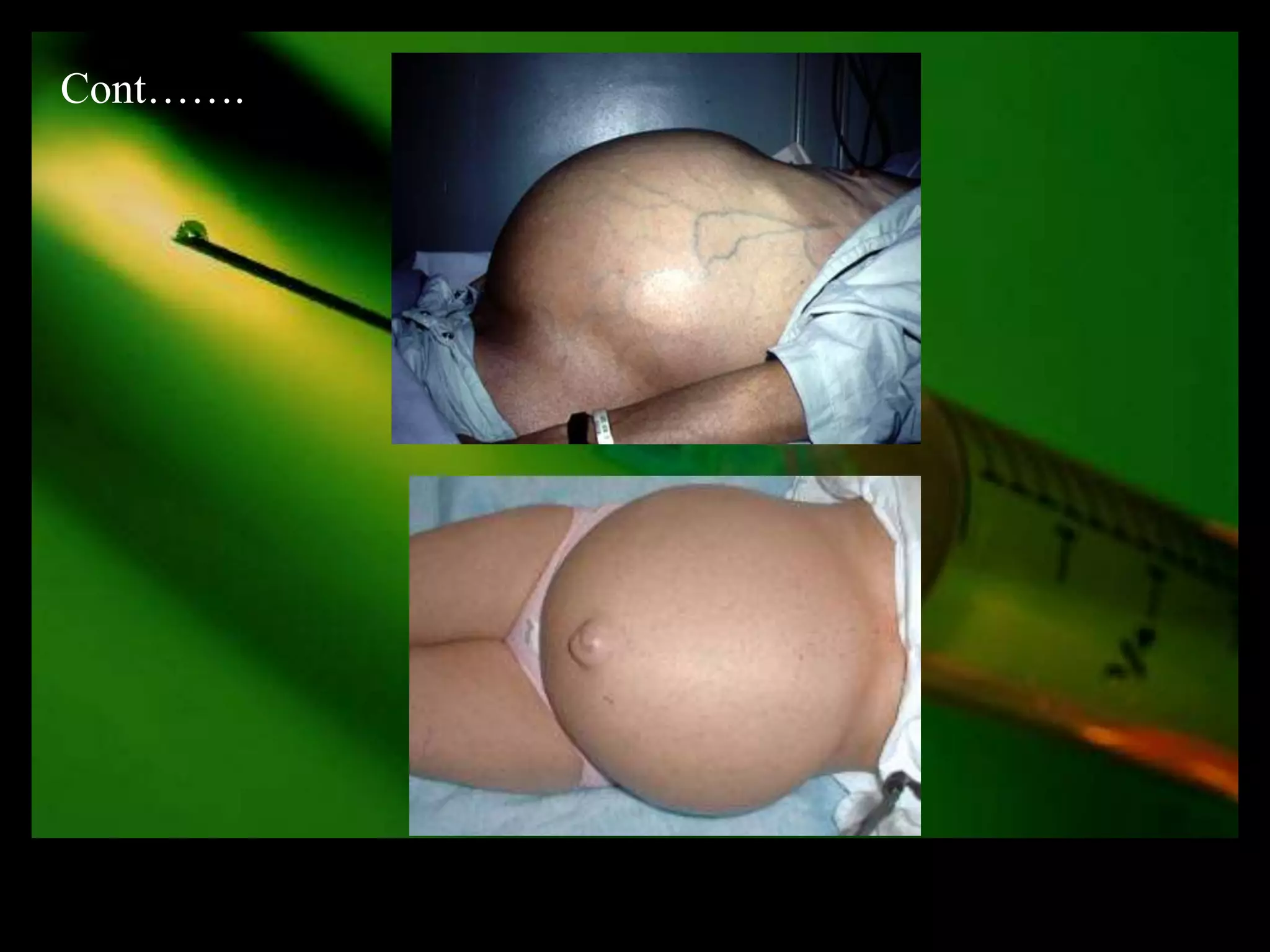



The document provides guidance on how to take a history and examine a patient presenting with edema. It discusses evaluating the appearance, onset, first site of appearance and associated symptoms to determine if the edema is localized or generalized. Examination of the patient should include assessing nutrition status, pallor, icterus, cyanosis, lymphadenopathy and vital signs. Demonstrating edema clinically involves applying pressure over bony prominences and looking for pitting. Specific examinations are described for cardiac, renal and ascites-related edema.































































































