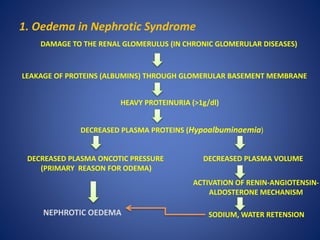
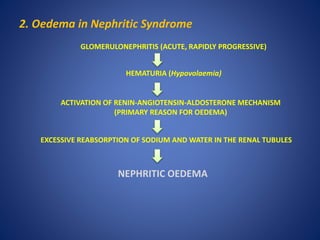
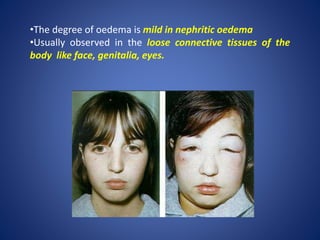
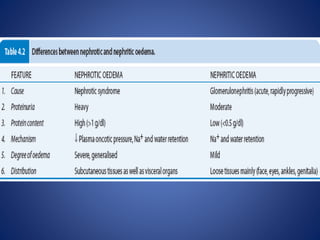
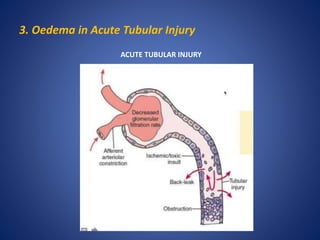
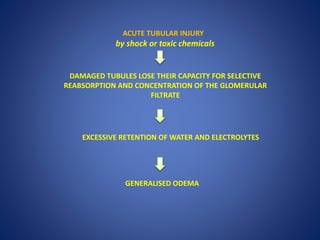
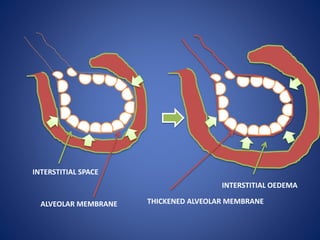
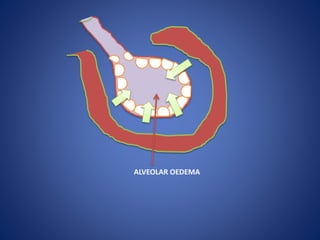
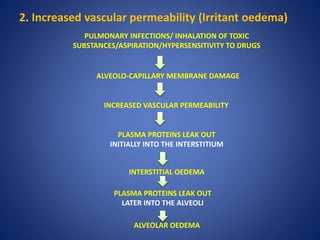
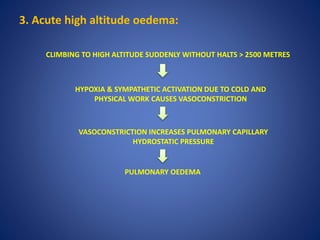
The document discusses different types of edema, including renal, cardiac, pulmonary, and cerebral edema. Renal edema can occur in nephrotic syndrome, nephritic syndrome, and acute tubular injury. Nephrotic edema is characterized by heavy proteinuria and hypoalbuminemia, while nephritic edema is caused by activation of the renin-angiotensin-aldosterone system. Cardiac edema develops due to heart failure, chronic hypoxia, or reduced cardiac output. Pulmonary edema can result from elevated pulmonary hydrostatic pressure, as in left heart failure, or increased capillary permeability due to infection, toxins, or altitude sickness.