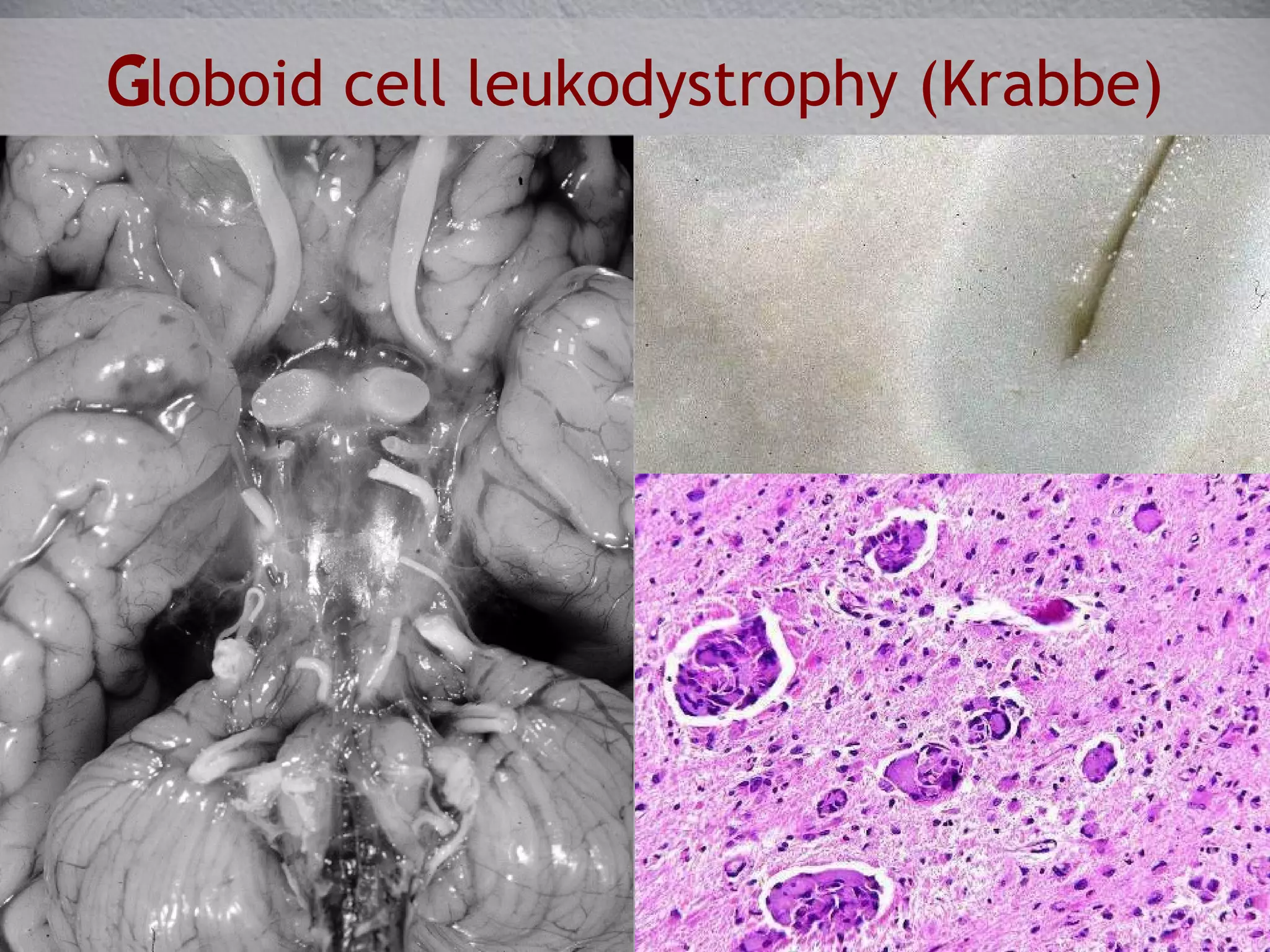
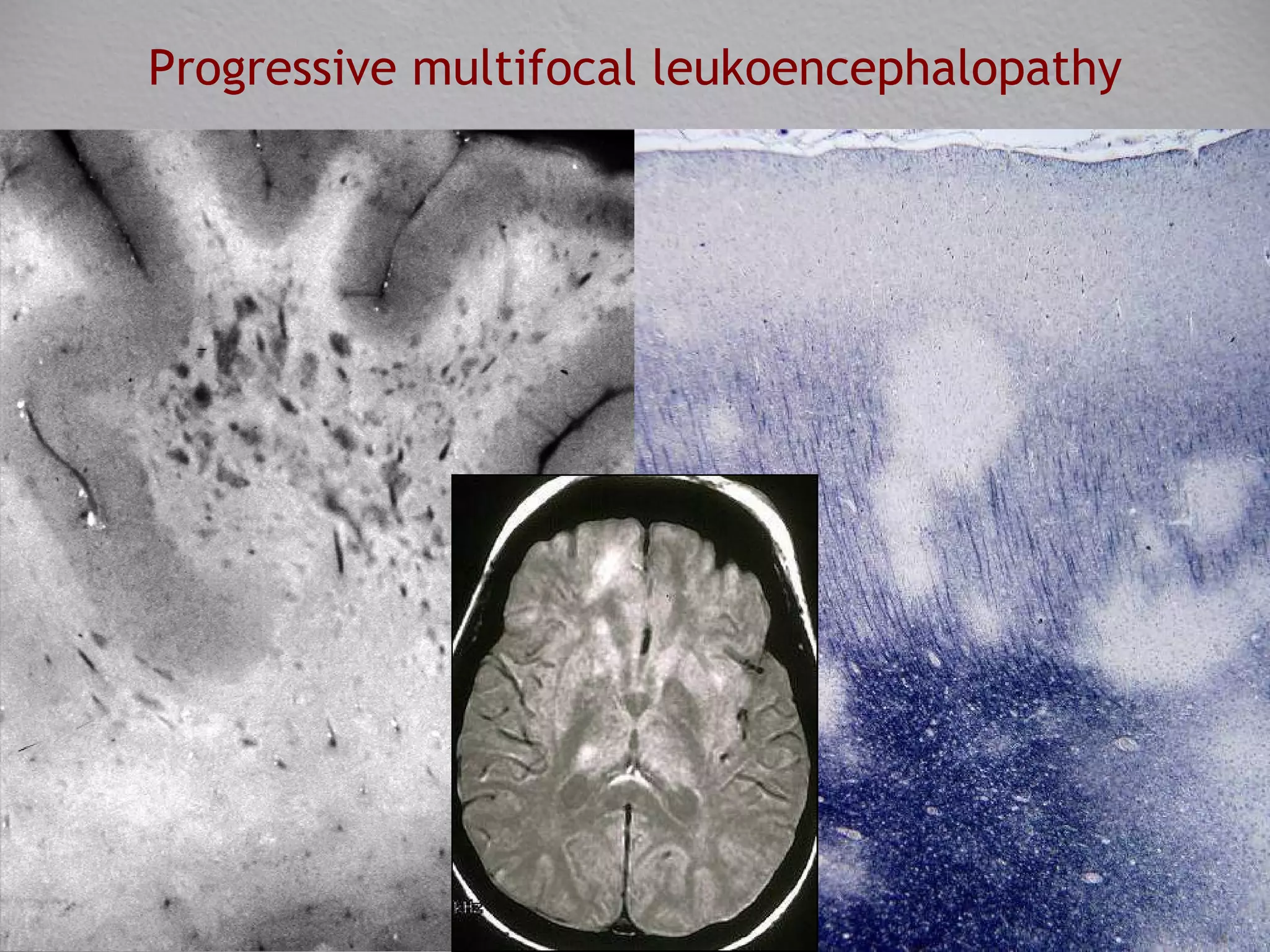
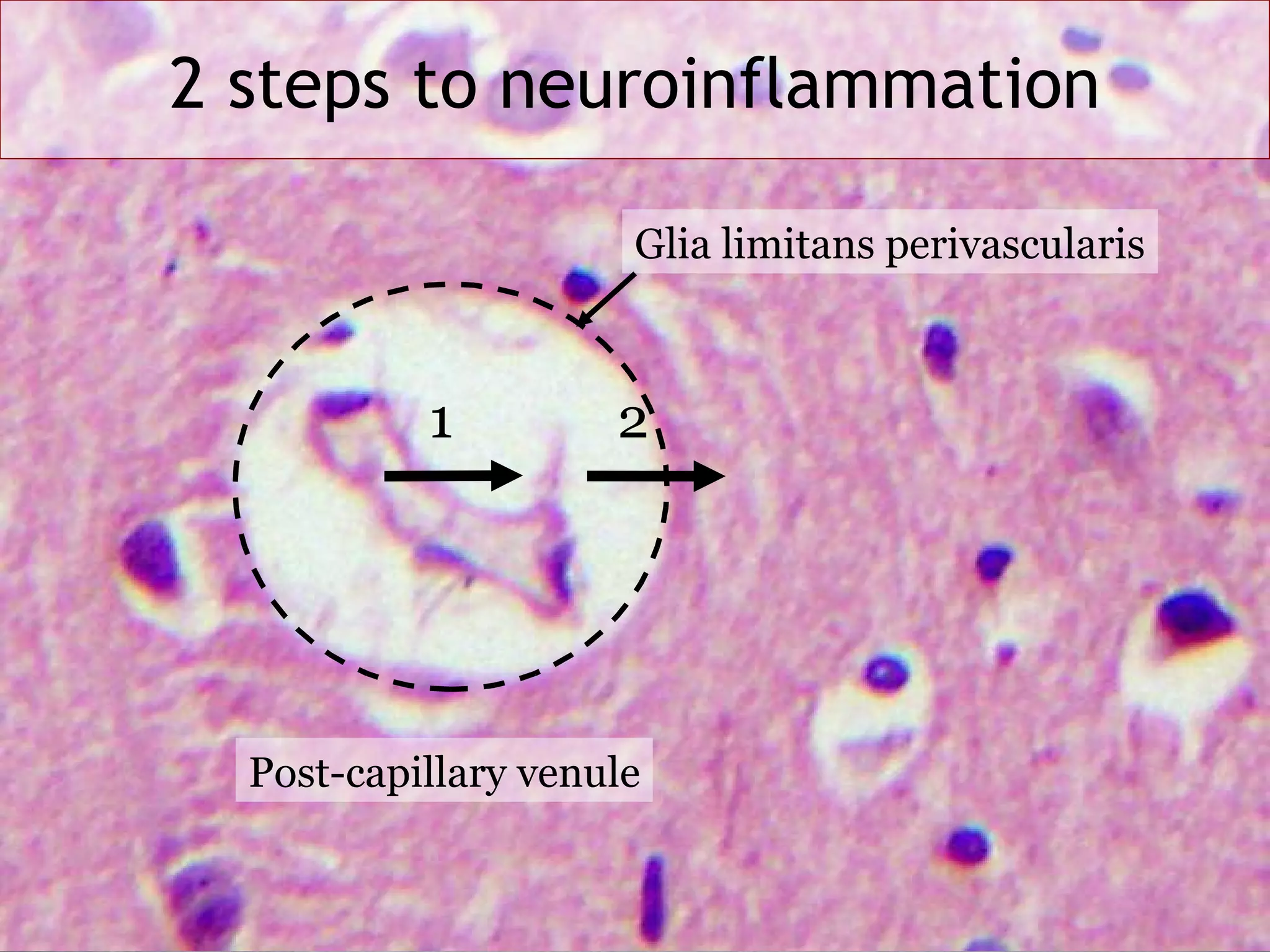
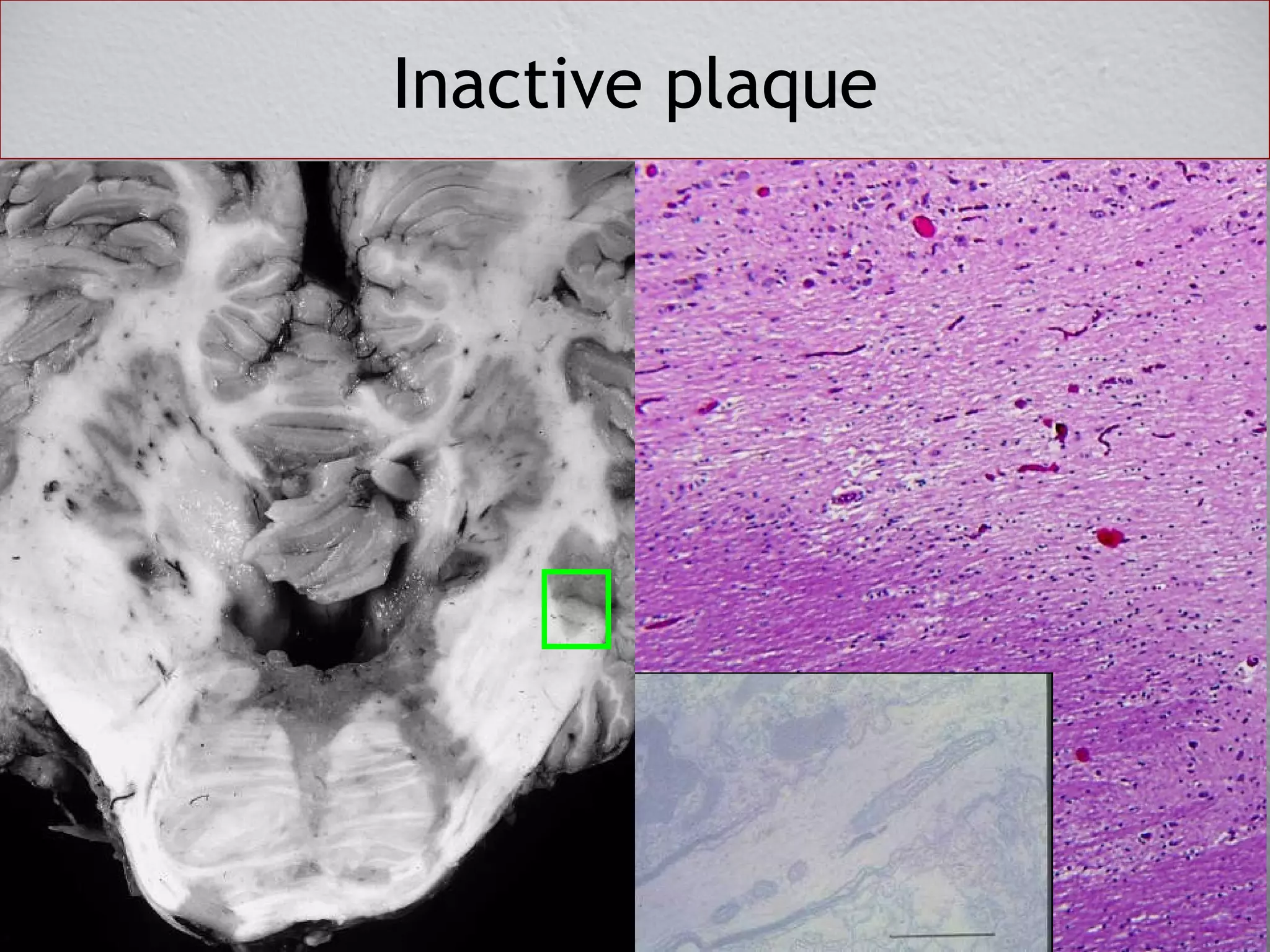
This document discusses demyelinating diseases that damage the white matter of the brain. It describes three major categories of leukoencephalopathies: genetic, acquired non-inflammatory, and acquired inflammatory. Genetic disorders include defects in lipid metabolism, cytoskeletal proteins, and myelin proteins. Acquired non-inflammatory disorders are toxic, metabolic, vascular or traumatic. Acquired inflammatory disorders include infectious diseases like HIV encephalitis and progressive multifocal leukoencephalopathy, as well as autoimmune diseases like multiple sclerosis. Multiple sclerosis involves inappropriate immune cell migration across the blood-brain barrier, leading to inflammation and damage to myelin, glia, axons and neurons.