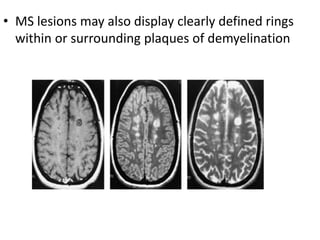
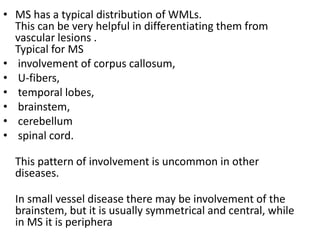
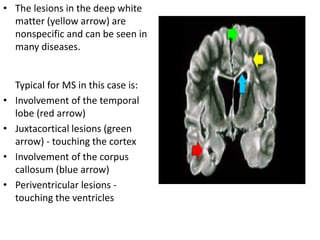
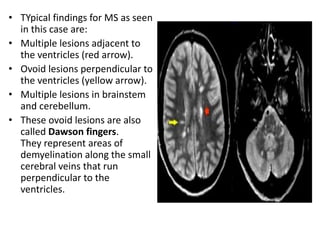
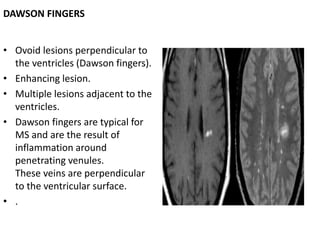
This document discusses multiple sclerosis and myelination. It begins by describing the differences between gray and white matter in the central nervous system. It then discusses how myelin is formed around axons by oligodendrocytes and the lipids and proteins that make up myelin. The document outlines the progression of myelination from birth through adulthood and the regions that myelinate first. It describes how myelination appears on MRI and classifies white matter diseases. Finally, it provides details on multiple sclerosis, including its pathology, clinical presentations, and use of MRI in diagnosis.
![Imaging
• MR has fundamentally changed the clinical evaluation of patients with
MS.
• The sensitivity of MR to MS lesions far exceeds that of the clinical
examination and any other imaging modality (e.g., computed
tomography [CT] .
• MR is not specific for the diagnosis of MS because white matter lesions
that mimic those of MS may be detected in both normal volunteers and
patients harboring other pathologic conditions, some of which have
nothing to do with demyelinating disease per se.
• Moreover, conventional MR can be normal in up to 25% of patients
with a proven clinical diagnosis
• . For these reasons, MR imaging cannot be the sole criterion for the
diagnosis of MS but must be included with clinical and laboratory
findings](https://image.slidesharecdn.com/ms-150108094505-conversion-gate02/85/imaging-of-multiple-sclerosis-25-320.jpg)





















































![Multiple sclerosis- Sushila [Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/multiplesclerosis-sushilaautosaved-230522133935-4f68df92-thumbnail.jpg?width=640&height=640&fit=bounds)




















