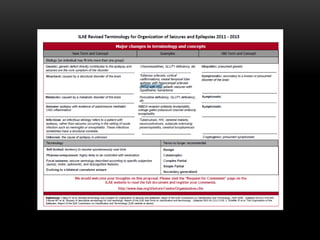
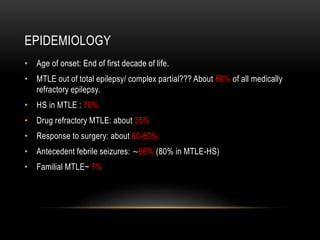
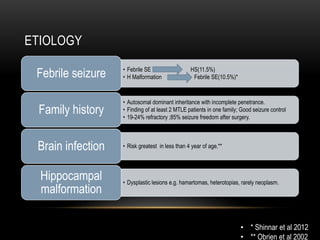
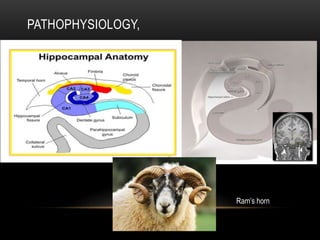
The document discusses mesial temporal lobe epilepsy (MTLE), including its history, epidemiology, etiology, pathophysiology, clinical presentation, diagnosis, and treatment. MTLE is characterized by seizures originating in the mesial temporal lobe and is often associated with hippocampal sclerosis that can be identified on MRI. Diagnosis involves a combination of clinical presentation, EEG, functional imaging like PET and SPECT, and sometimes invasive monitoring to localize the seizure focus.








































![mts[1] the important cause of epilepsy.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/mts1-250410163942-19d8a3ca-thumbnail.jpg?width=640&height=640&fit=bounds)





























