
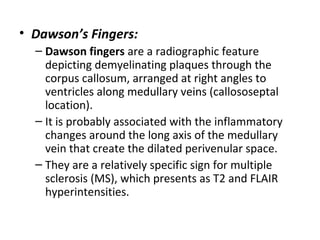
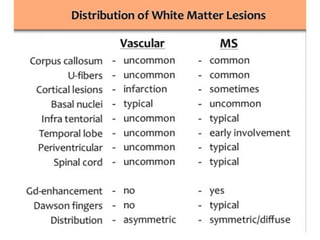
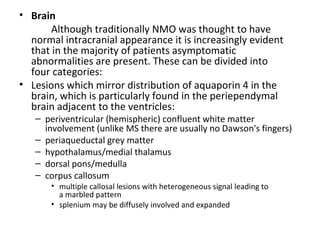
![MAGNETIC RESONANCE
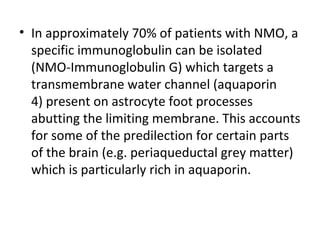
IMAGING
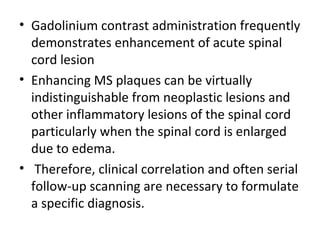
• MRI has revolutionised the diagnosis and surveillance of patients with MS.
• The sensitivity of MR to MS lesions far exceeds that of the clinical
examination and any other imaging modality (e.g., computed tomography
[CT] .
• MR is not specific for the diagnosis of MS because white matter lesions
that mimic those of MS may be detected in both normal volunteers and
patients harboring other pathologic conditions, some of which have
nothing to do with demyelinating disease per se.
• Moreover, conventional MR can be normal in up to 25% of patients with a
proven clinical diagnosis
• For these reasons, MR imaging cannot be the sole criterion for the
diagnosis of MS but must be included with clinical and laboratory findings](https://image.slidesharecdn.com/imagingofdemyelinatingdiseasesfinal-151209173535-lva1-app6892/85/Imaging-of-demyelinating-diseases-final-35-320.jpg)
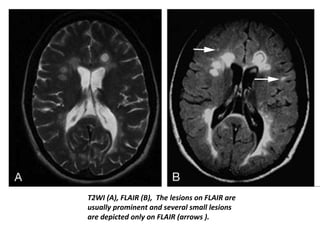
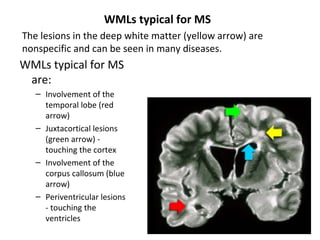
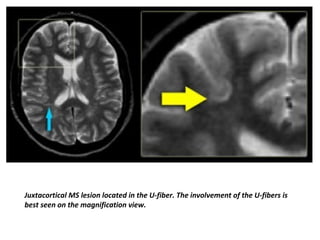
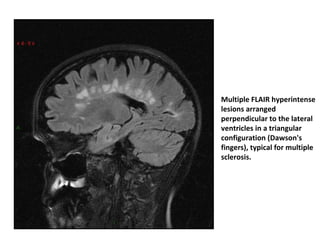
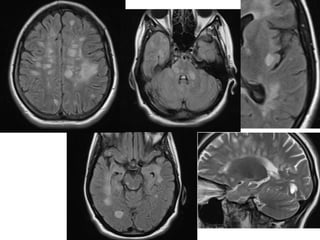
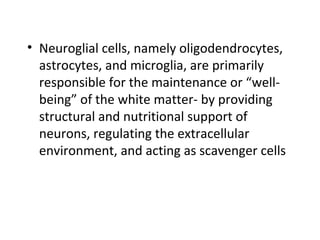
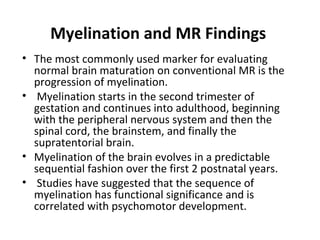
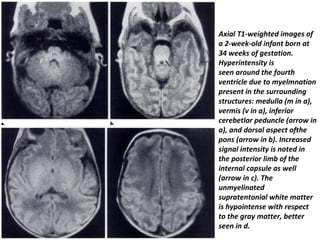
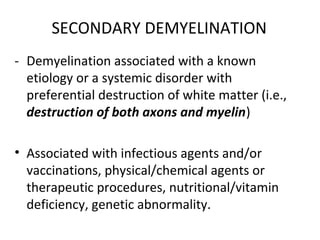
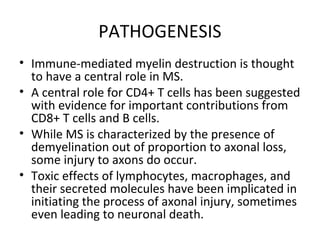
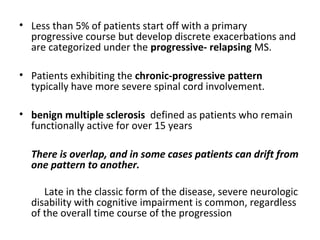
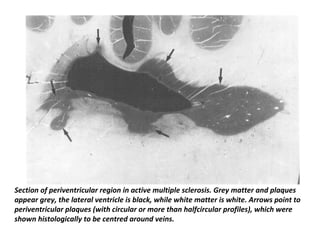
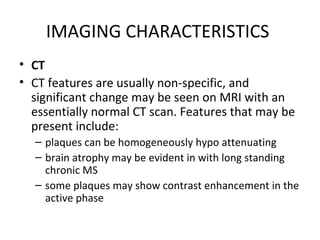
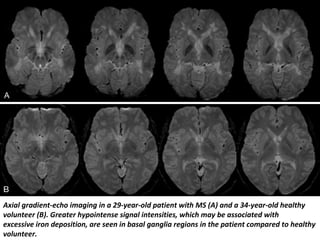
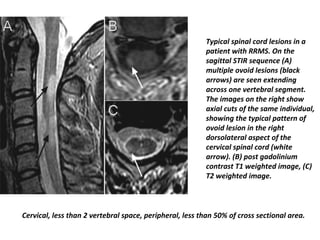
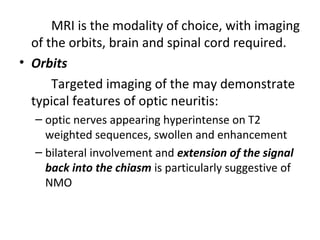
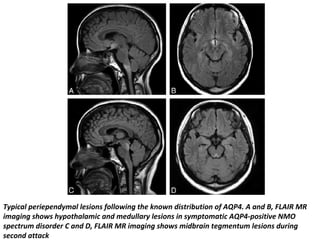
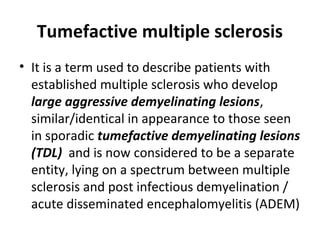
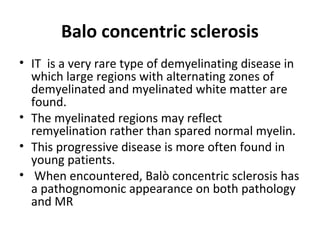
![Intermediate-weighted [IW] , T2-weighted) , FLAIR and three-dimensional double-
inversion-recovery(DIR) images of intracortical lesions. Lesion (arrowhead) in cortical
gray matter, with a possible juxtacortical component is shown. The intracortical lesion
is particularly poorly visible on intermediate-weighted and T2-weighted images, as well
as on the FLAIR image, whereas it is depicted clearly on the double-inversion-recovery
image..](https://image.slidesharecdn.com/imagingofdemyelinatingdiseasesfinal-151209173535-lva1-app6892/85/Imaging-of-demyelinating-diseases-final-68-320.jpg)
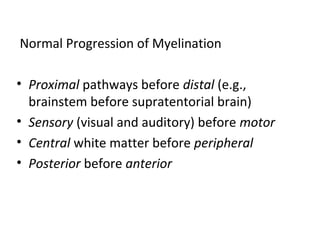
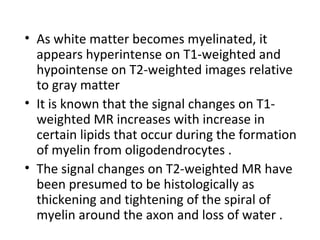
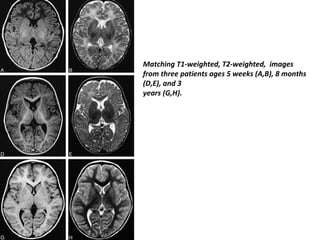
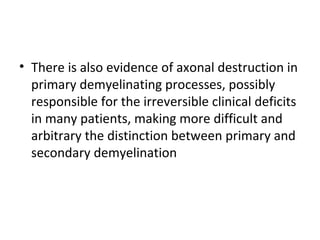
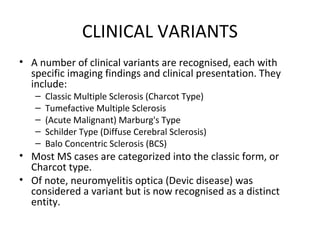
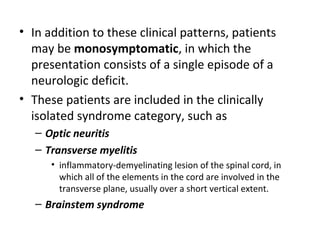
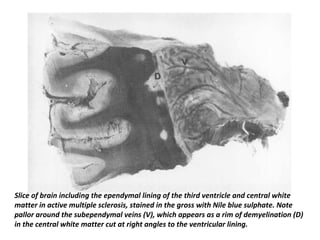
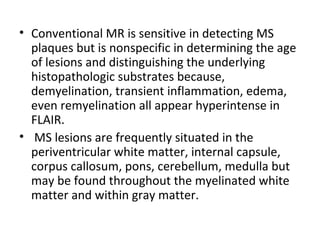
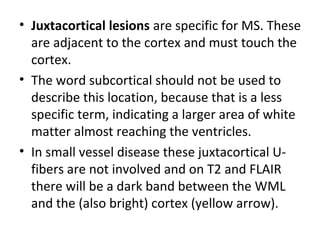
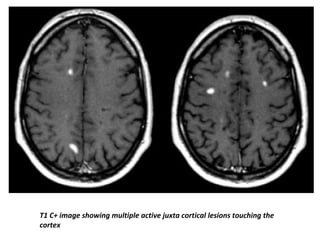
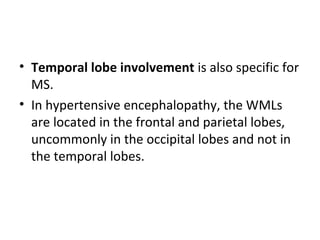
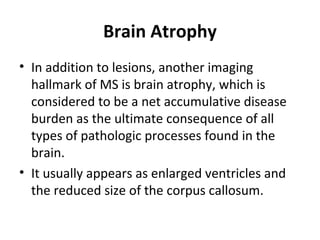
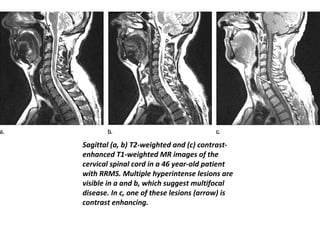
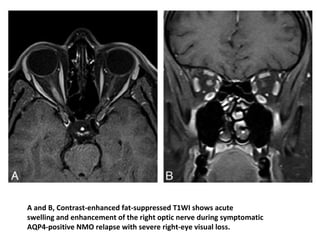
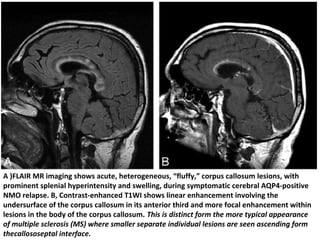
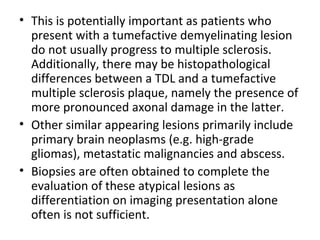
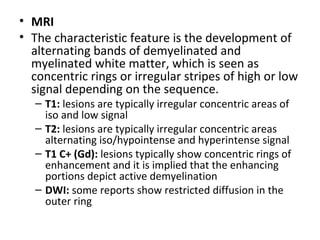
![Intermediate-weighted [IW] , T2-weighted) , FLAIR and three-
dimensional double-inversion-recovery(DIR) images of intracortical
lesions. In a different patient, double-inversion-recovery image
shows very good delineation of intracortical lesion (arrowhead), which
may be mistaken for a juxtacortical lesion or a partial
volume artifact on the T2-weighted image and may even be missed on
the FLAIR image](https://image.slidesharecdn.com/imagingofdemyelinatingdiseasesfinal-151209173535-lva1-app6892/85/Imaging-of-demyelinating-diseases-final-69-320.jpg)
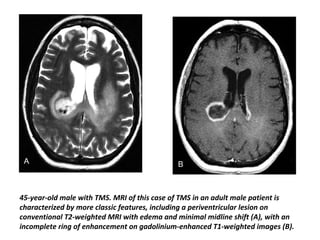


This document discusses pathology and imaging of multiple sclerosis. It begins by describing the composition and development of myelin and white matter in the central nervous system. It then discusses multiple sclerosis as a primary demyelinating disease characterized by plaques seen on imaging. The clinical manifestations and variants of multiple sclerosis are described. Imaging findings on CT, MRI, T1-weighted, T2-weighted, and FLAIR sequences are provided, showing the appearance of lesions in white matter and ability to detect acute inflammation.

































































![Multiple sclerosis- Sushila [Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/multiplesclerosis-sushilaautosaved-230522133935-4f68df92-thumbnail.jpg?width=640&height=640&fit=bounds)




























