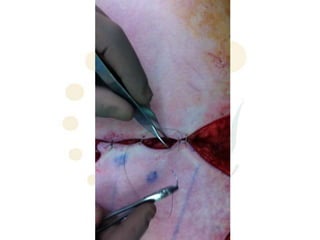
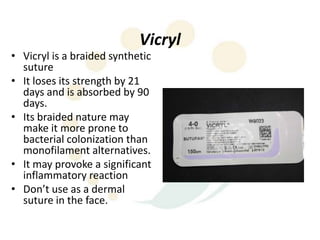
The document provides guidance on suturing techniques. It recommends everting the skin edges when suturing to achieve better dermal apposition, improved healing, and a finer scar. A triangular suture passage with the base located deeply is suggested to evert the wound edges, while an inverted triangular shape tends to invert them. Dermal sutures are recommended first to reduce tension before cutaneous sutures. Adjusting where the knot lies can help flatten steps between uneven wound edges. The document also reviews appropriate suture materials for different areas, recommending absorbable sutures that elicit minimal tissue reaction for the face and longer-absorbing sutures for prone areas like the back.