Downloaded 1,663 times




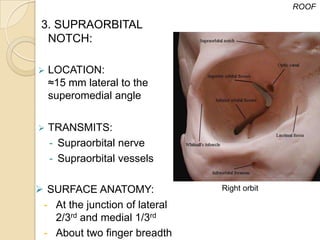




Palpable just above the orbital rim - Can be easily felt - Landmark for localizing supraorbital notch - Supraorbital nerve block can be given here - Site for incision in supraorbital approach - Fractures commonly involve this area - Site for Botox injection for eyebrow lifting - Site for incision in browlift surgery - Site for incision in supraorbital nerve block - Site for incision in supraorbital approach






























































































