Download as PDF, PPTX

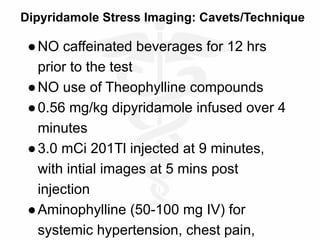
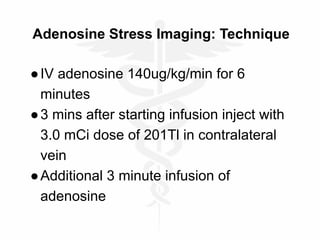
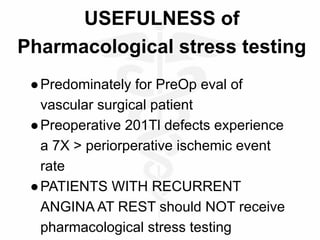
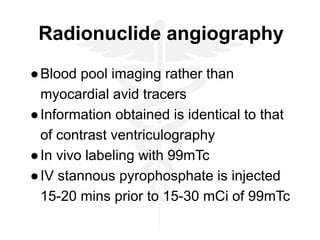


Nuclear cardiology uses radiolabeled tracers and imaging techniques to provide functional data on cardiac physiology. Common studies include myocardial perfusion imaging using thallium-201 or technetium-99m to evaluate blood flow and ischemia. Gated blood pool imaging with technetium-99m allows assessment of ejection fraction and wall motion. Myocardial infarction can be identified using radiolabeled antibodies that localize to injured heart muscle. Positron emission tomography provides metabolic data to evaluate hibernating myocardium. Overall, nuclear cardiology noninvasively evaluates cardiac function and identifies ischemia, scar, and viability.













































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)