● Novel SPECTScanners
Innovative Gantry - Cadiofocal / 3600
detection
SSD - convert photons directly to electrons, Replacing the need
for bulky photomultipliers
Cardiocentric Design - 5x count sensitivity, 2x spatial resolution
Rapid Protocol or Low Radiation Protocol
Seated Position
Dynamic Imaging and MBF quantification - Complete
tomography data acquired simultaneously
9.
Image Acquisition
● 4modes : list mode, static mode, ECG gated and dynamic.
● List mode - information stored for every detected event
Reconstructed as a static image or dynamic image series for
absolute quantification of radiotracer concentration in tissues
● ECG gated images allow assessment of RWMA, LV volumes,
Ventricular dyssynchrony
● Dynamic imaging - tracks the radiotracer through blood vessels
and heart starting with injection
● Myocardial blood flow estimates can be derived - rest / stress.
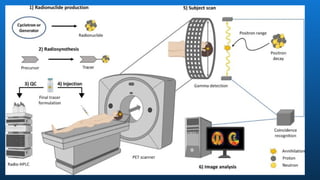
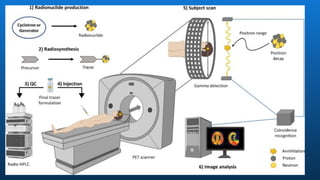
Working Principle
● Quantificationof Radioactivity in vivo
● IV injection of a positron-emitting radiopharmaceutical
● Undergoes B+
-> Neutrino and Positron
● Positron collides( Annihilates) with an electron
● Producing 2 Photons
● Photons detected by Detectors
13.
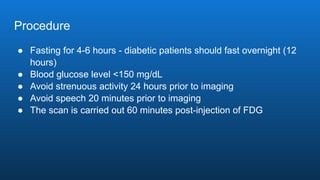
Procedure
● Fasting for4-6 hours - diabetic patients should fast overnight (12
hours)
● Blood glucose level <150 mg/dL
● Avoid strenuous activity 24 hours prior to imaging
● Avoid speech 20 minutes prior to imaging
● The scan is carried out 60 minutes post-injection of FDG
16.
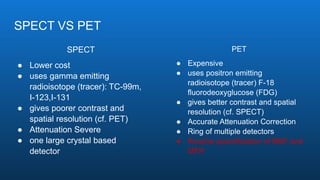
SPECT VS PET
SPECT
●Lower cost
● uses gamma emitting
radioisotope (tracer): TC-99m,
I-123,I-131
● gives poorer contrast and
spatial resolution (cf. PET)
● Attenuation Severe
● one large crystal based
detector
PET
● Expensive
● uses positron emitting
radioisotope (tracer) F-18
fluorodeoxyglucose (FDG)
● gives better contrast and spatial
resolution (cf. SPECT)
● Accurate Attenuation Correction
● Ring of multiple detectors
● Routine quantification of MBF and
MFR
17.
Working Principle
● Quantificationof Radioactivity in vivo
● IV injection of a positron-emitting radiopharmaceutical
● Undergoes B+
-> Neutrino and Positron
● Positron collides( Annihilates) with an electron
● Producing 2 Photons
● Photons detected by Detectors
19.
Procedure
● Fasting for4-6 hours - diabetic patients should fast overnight (12
hours)
● Blood glucose level <150 mg/dL
● Avoid strenuous activity 24 hours prior to imaging
● Avoid speech 20 minutes prior to imaging
● The scan is carried out 60 minutes post-injection of FDG
22.
SPECT VS PET
SPECT
●Lower cost
● uses gamma emitting
radioisotope (tracer): TC-99m,
I-123,I-131
● gives poorer contrast and
spatial resolution (cf. PET)
● Attenuation Severe
● one large crystal based
detector
PET
● Expensive
● uses positron emitting
radioisotope (tracer) F-18
fluorodeoxyglucose (FDG)
● gives better contrast and spatial
resolution (cf. SPECT)
● Accurate Attenuation Correction
● Ring of multiple detectors
● Routine quantification of MBF and
MFR
23.
Hybrid SPECT/CT, PET/CT,and PET/MRI
● Integrated CT gantry
● CT images can be used for attenuation correction, quantification of
coronary artery calcium, and/or coronary angiography.
● PET/MRI - Research purposes
Attenuation correction difficult
Advantage of respiratory motion compensation and simultaneous
imaging of dual physiological processes.
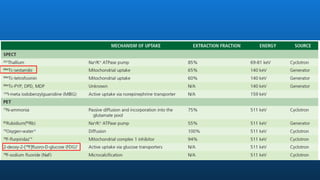
99mTc-sestamibi
● FDA approvedSPECT tracer
● Half live 6 hrs ( compared to 72hrs of 201
thallium)
● Emits high energy - 140 keV gamma rays ( vs 80 Kev of 201
thallium)
● Available as unit doses - increasing accessibility
● Suitable for exercise or pharmacological stress testing
● Lesser radiation dose than 201
thallium
● Currently 201
Thallium is no longer recommended unless used for viability
assessment in centres with no PET
28.
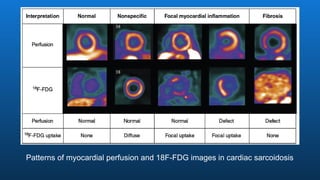
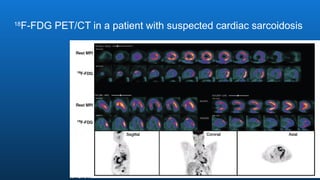
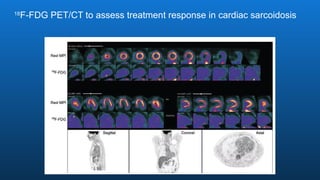
2-deoxy-2-[18F]fluoro-D-glucose(FDG)
● Myocardial metabolicimaging tracer
● Image myocardial glucose metabolism
● 18F-FDG - enters myocardial cells through GLUT 1 and GLUT 4
● Insulin, ischemia, and hypoxia induce translocation of GLUT to the
plasma membrane and increase myocyte glucose uptake.
● Ischemic cells and Hypoxic cells overexpress GLUT’s and
primarily use glucose for metabolism
● Malignant cells and Inflammatory cells have increased glucose
uptake by insulin independent mechanisms.
29.
● Dietary manipulation-> Forces the myocardial metabolism to switch
to use either glucose or fatty acids.
● Forms the basis for the requirement of dietary modification for
different scans
- Myocardial Viability -> glucose load with IV insulin
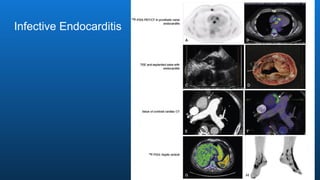
- Cardiovascular inflammatory conditions(eg: sarcoidosis, infective
endocarditis, and vasculitis) -> low-carbohydrate, high-fat diet
followed by prolonged fasting
30.
Patient Preparation beforeMPI
● Stress Testing
- 6 hrs fasting
- No smoking for prior 6 hrs
- Caffeine withheld for 12 hrs
- Theophylline containing medications w/h for 48 hrs
- K/C/O CAD - on antianginal medications
- Not a K/C/O CAD - withhold antianginals and BB for 12 hrs
- HD patients - Test one day after HD
31.
Patient Preparation beforeMPI ( Continued…)
● 18
F-FDG for Viability
- 6h fast
- RBS checked on arrival
- Glucose drink given
- 45 mins later -> IV insulin given to drive RBS <150 mg/dl
● 18
F-FDG for Inflammation / Infection
- High Fat / low - zero carb diet x 2 large meals 24 hrs before the test
- Overnight fast 8 - 12 hrs
● Amyloidosis Imaging and Gated Blood Pool Scans
No specific dietary preparation is necessary - 99mTc-pyrophosphate,
DPD, or HMDP imaging
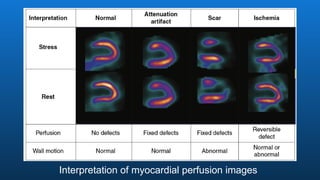
IHD
● Principle fordetecting CAD on MPI : ability of a radiotracer to identify a transient
regional perfusion deficit in a myocardial region subtended by a coronary artery with a
flow-limiting stenosis
● Reversible MPD -> Ischemia
● Fixed MPD -> Scar from prior MI
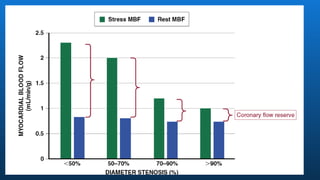
● MPD during stress -> develop downstream to a epicardial stenosis with ≥50% to 70%
luminal narrowing and become progressively more severe with increasing degree of
stenosis.
● Lesions with intermediate stenosis ( 50% - 90%) are associated with significant
variablitiy in maximal MBF -> severity of MPD
● Multitude of factors contribute to the disagreements between angiographically defined
CAD and its associated physiologic severity by radionuclide perfusion imaging
39.
Suspected CAD -Pts with new onset chest pain
● Excellent choice especially in older patients where calcified coronary arteries
are expected ( compared to CTA in younger pts)
● A large meta analysis of 86 studies (10.8K pts )
pooled sensitivity - 87% and specificity - 78%
● Recent Meta analyses - EVINCI and PACIFIC - PET MPI is one of the most
accurate noninvasive techniques for detecting flow-limiting CAD.
● an MFR >2.0 is associated with a >97% negative predictive value for ruling
out high-risk angiographic CAD.
40.
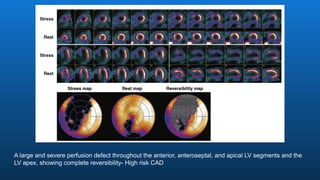
Case -1
● 80-year-oldman presenting with atypical chest pain and dyspnea.
● Exercise was terminated because of chest pain, with associated decrease in
blood pressure and 3-mm downsloping ST-segment depression in the
inferolateral leads
● There was also a decrease in LV ejection fraction after exercise
41.
A large andsevere perfusion defect throughout the anterior, anteroseptal, and apical LV segments and the
LV apex, showing complete reversibility- High risk CAD
42.
Case 2
● 85-year-old woman presenting with exertional dyspnea
● Rest and vasodilator-stress 82
rubidium position emission tomography scan
done
43.
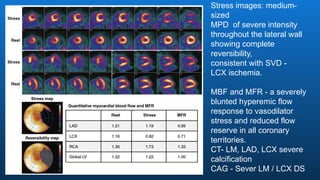
Stress images: medium-
sized
MPDof severe intensity
throughout the lateral wall
showing complete
reversibility,
consistent with SVD -
LCX ischemia.
MBF and MFR - a severely
blunted hyperemic flow
response to vasodilator
stress and reduced flow
reserve in all coronary
territories.
CT- LM, LAD, LCX severe
calcification
CAG - Sever LM / LCX DS
45.
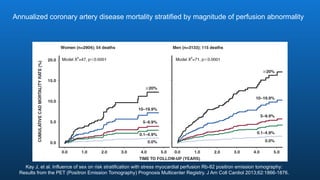
Kay J, etal. Influence of sex on risk stratification with stress myocardial perfusion Rb-82 positron emission tomography:
Results from the PET (Positron Emission Tomography) Prognosis Multicenter Registry. J Am Coll Cardiol 2013;62:1866-1876.
Annualized coronary artery disease mortality stratified by magnitude of perfusion abnormality
46.
● Coronary microvasculardysfunction (CMD ) is quite common in symptomatic
patients with RF.
● Women > Men
● Symptomatic CMD pts have worse prognosis than asypmtomatic pts.
● PET imaging is considered the most accurate and reproducible noninvasive
technique.
● Reduction in stress CBF and MFR reflect combined effects of altered fluid
dynamics caused by diffuse atherosclerosis and microcirculatory dysfucntion
● Diffuse nonobstructive CAD is a common finding in symptomatic patients with
CMD and can be identified using coronary artery calcium scoring.
Suspected CAD - Symptomatic Pts w/o Angiographic
Obstructive CAD
47.
Case -3
● 76-year-old woman with dyslipidemia, hypertension, and nonobstructive
angiographic coronary artery disease presented with atypical chest pain and
dyspnea.
48.
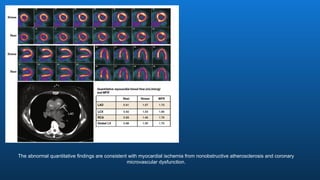
The abnormal quantitativefindings are consistent with myocardial ischemia from nonobstructive atherosclerosis and coronary
microvascular dysfunction.
49.
Evaluation Before OrganTransplantation
● CKD for Kidney Transplant
● Younger patients CTA is a reasonable test
● Pts > 55 ys with CKD - non invasive stress testing reasonable
● Number of studies showed that abnormal MPI is associated with both short-
and long-term adverse cardiac events in CKD pts including renal transplant
patients, and that a normal MPI study has a high negative predictive value.
50.
Suspected ACS -Nondiagnostic ECG and Hs Trop +
● In intermediate-high risk patients with low-level elevation of cardiac troponin,
quantitative stress PET perfusion imaging may offer an advantage compared
with SPECT and may be preferable if available.
● In one study - Impaired global MFR in the absence of obstructive CAD as
measured by PET was independently associated with troponin elevation,
● ? association between chronic microvascular ischemia and myocardial injury,
especially among patients with diffuse atherosclerosis
51.
Patient with priorPCI and Recurrent Symptoms
● Radionuclide MPI is appropriate for diagnosis of ischemia and risk
stratification among patients with prior revascularization presenting
with new-onset or worsening symptoms of angina or anginal equivalents.
● Pts with prior PCI / CABG - MPI provides localization and quantification of
myocardial ischemia that helps with risk prediction and management
decisions regarding the potential need for targeted revascularization
● Exercise test ideal
● PET > specificity SPECT, & higher diagnostic accuracy.
52.
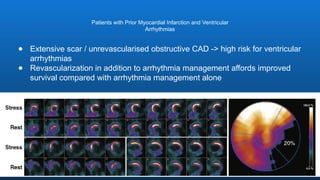
● Extensive scar/ unrevascularised obstructive CAD -> high risk for ventricular
arrhythmias
● Revascularization in addition to arrhythmia management affords improved
survival compared with arrhythmia management alone
Patients with Prior Myocardial Infarction and Ventricular
Arrhythmias
53.
Patients with CTO
●CTO - prevalence rate estimated between 18% and 52%.
● In experienced centers, CTO PCI may substantially reduce myocardial
ischemia and improve quality of life.
● Demonstration of significant myocardial ischemia and viability within the
territory supplied by a coronary vessel with a CTO is generally accepted as a
useful approach to help inform the risk versus benefit of CTO PCI.
55.
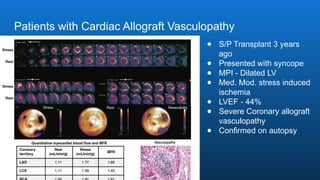
Patients with CardiacAllograft Vasculopathy
● S/P Transplant 3 years
ago
● Presented with syncope
● MPI - Dilated LV
● Med. Mod. stress induced
ischemia
● LVEF - 44%
● Severe Coronary allograft
vasculopathy
● Confirmed on autopsy
56.
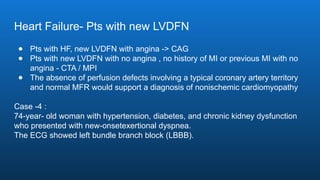
Heart Failure- Ptswith new LVDFN
● Pts with HF, new LVDFN with angina -> CAG
● Pts with new LVDFN with no angina , no history of MI or previous MI with no
angina - CTA / MPI
● The absence of perfusion defects involving a typical coronary artery territory
and normal MFR would support a diagnosis of nonischemic cardiomyopathy
Case -4 :
74-year- old woman with hypertension, diabetes, and chronic kidney dysfunction
who presented with new-onsetexertional dyspnea.
The ECG showed left bundle branch block (LBBB).
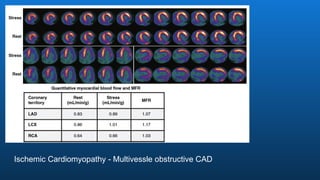
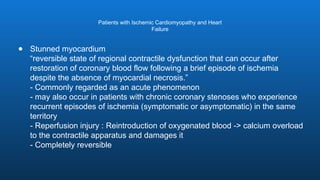
Patients with IschemicCardiomyopathy and Heart
Failure
● Stunned myocardium
“reversible state of regional contractile dysfunction that can occur after
restoration of coronary blood flow following a brief episode of ischemia
despite the absence of myocardial necrosis.”
- Commonly regarded as an acute phenomenon
- may also occur in patients with chronic coronary stenoses who experience
recurrent episodes of ischemia (symptomatic or asymptomatic) in the same
territory
- Reperfusion injury : Reintroduction of oxygenated blood -> calcium overload
to the contractile apparatus and damages it
- Completely reversible
60.
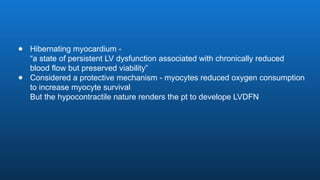
● Hibernating myocardium-
“a state of persistent LV dysfunction associated with chronically reduced
blood flow but preserved viability”
● Considered a protective mechanism - myocytes reduced oxygen consumption
to increase myocyte survival
But the hypocontractile nature renders the pt to develope LVDFN
61.
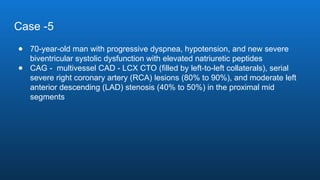
Case -5
● 70-year-oldman with progressive dyspnea, hypotension, and new severe
biventricular systolic dysfunction with elevated natriuretic peptides
● CAG - multivessel CAD - LCX CTO (filled by left-to-left collaterals), serial
severe right coronary artery (RCA) lesions (80% to 90%), and moderate left
anterior descending (LAD) stenosis (40% to 50%) in the proximal mid
segments
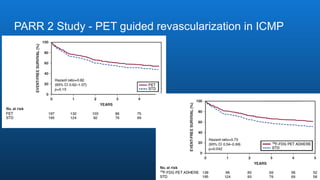
63.
PARR 2 Study- PET guided revascularization in ICMP







![2-deoxy-2-[18F]fluoro-D-glucose(FDG)
● Myocardial metabolic imaging tracer
● Image myocardial glucose metabolism
● 18F-FDG - enters myocardial cells through GLUT 1 and GLUT 4
● Insulin, ischemia, and hypoxia induce translocation of GLUT to the
plasma membrane and increase myocyte glucose uptake.
● Ischemic cells and Hypoxic cells overexpress GLUT’s and
primarily use glucose for metabolism
● Malignant cells and Inflammatory cells have increased glucose
uptake by insulin independent mechanisms.](https://image.slidesharecdn.com/mpimyocardialperfusionimaging1-250220192415-6e8db0fa/85/MPI-Myocardial-Perfusion-Imaging-1-pptx-28-320.jpg)