Downloaded 648 times

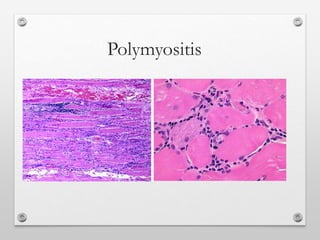
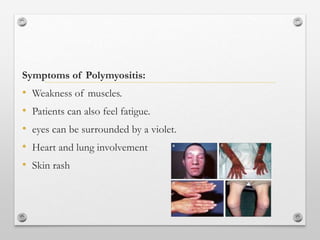

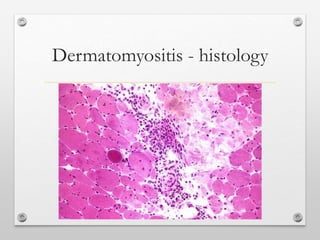

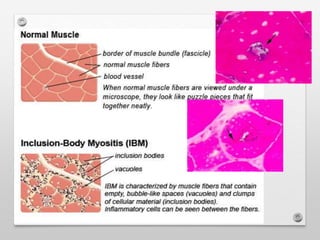
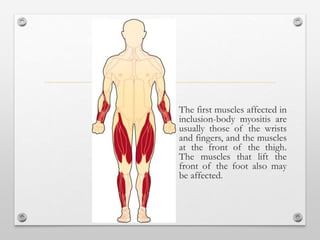
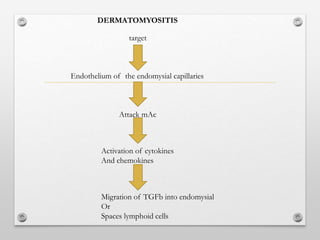
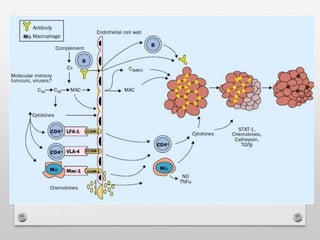
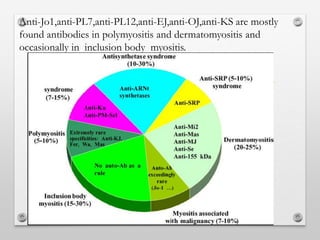


The document discusses various types of inflammatory myopathies (myositis): 1) Polymyositis causes symmetric proximal muscle weakness and inflammation within muscle fibers. Symptoms include fatigue and a skin rash. 2) Dermatomyositis causes similar muscle symptoms but also features a characteristic rash on the skin. It can also involve other organs. 3) Inclusion body myositis typically causes asymmetric weakness of wrist, finger, and thigh muscles. It involves degeneration in addition to immune dysfunction. 4) Overlap myositis combines myopathy with connective tissue diseases like lupus. Diagnosis involves blood tests, muscle enzyme levels, muscle biopsy and MRI or EMG. Treatment
















































































