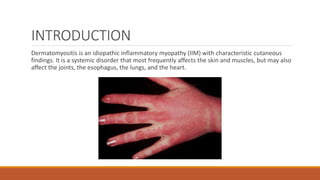
Dermatomyositis is an inflammatory myopathy that affects the skin and muscles. It is characterized by progressive proximal symmetrical muscle weakness, elevated muscle enzyme levels, abnormal electromyography and muscle biopsy findings. The cause is unknown but may involve genetic, immunological, infectious or environmental factors. Diagnosis involves assessing muscle symptoms, rashes and laboratory tests showing muscle inflammation. Treatment focuses on sun protection, immunosuppressants like hydroxychloroquine and methotrexate, and corticosteroids. Lifestyle measures like diet, activity and sun avoidance are also important.
![ETIOLOGY
Infectious agents have been suggested as possible triggers of dermatomyositis. These include
the following:
• Viruses (eg, coxsackievirus, parvovirus, echovirus, human T-cell lymphotropic virus type 1
[HTLV-1], HIV)
• Toxoplasma species
• Borrelia species](https://image.slidesharecdn.com/dermatomyositis-211206185859/85/Dermatomyositis-5-320.jpg)

![LABORATORY DIAGNOSIS
Muscle enzyme levels are often abnormal during the course of dermatomyositis, except in
patients with amyopathic dermatomyositis (ADM). The most sensitive/specific enzyme
abnormality is elevated creatine kinase (CK), but aldolase studies and other tests (eg, for
aspartate aminotransferase [AST] or lactic dehydrogenase [LDH]) may also yield abnormal results.](https://image.slidesharecdn.com/dermatomyositis-211206185859/85/Dermatomyositis-11-320.jpg)