Downloaded 1,921 times
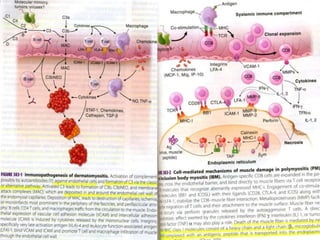

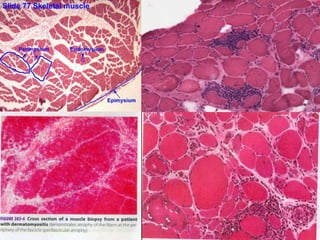



Myopathy refers to primary skeletal muscle dysfunction, which can manifest through various symptoms including muscle wasting, pain, and involuntary contractions. This document categorizes myopathies into several types, emphasizing inflammatory myopathies as the largest group, detailing their pathogenesis, clinical features, diagnostic processes, and treatment options. The document outlines the importance of proper diagnosis through muscle biopsy and electromyography, highlighting that conditions like polymyositis and dermatomyositis often respond well to treatment, while inclusion body myositis poses a more challenging prognosis.























































































