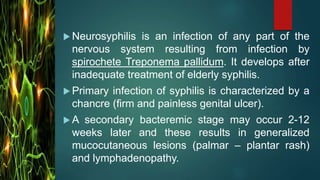
Neurosyphilis is an infection of the nervous system caused by the bacterium Treponema pallidum, which causes syphilis. It typically develops after many years of untreated syphilis. Symptoms vary depending on the areas affected but may include mental deterioration, paralysis, meningitis, tabes dorsalis resulting in girdle pain and joint damage, and ocular symptoms. Treatment involves intravenous penicillin, but neurosyphilis can still cause permanent damage. Nursing care focuses on maintaining patient health, safety, and independence through measures like seizure precautions, skin care, physiotherapy, and partner screening.





















































![Neuropsychiatry [2017]](https://cdn.slidesharecdn.com/ss_thumbnails/neuropsychiatricmanifestationofcommonneurologicaldisorders-171001003940-thumbnail.jpg?width=640&height=640&fit=bounds)





















































