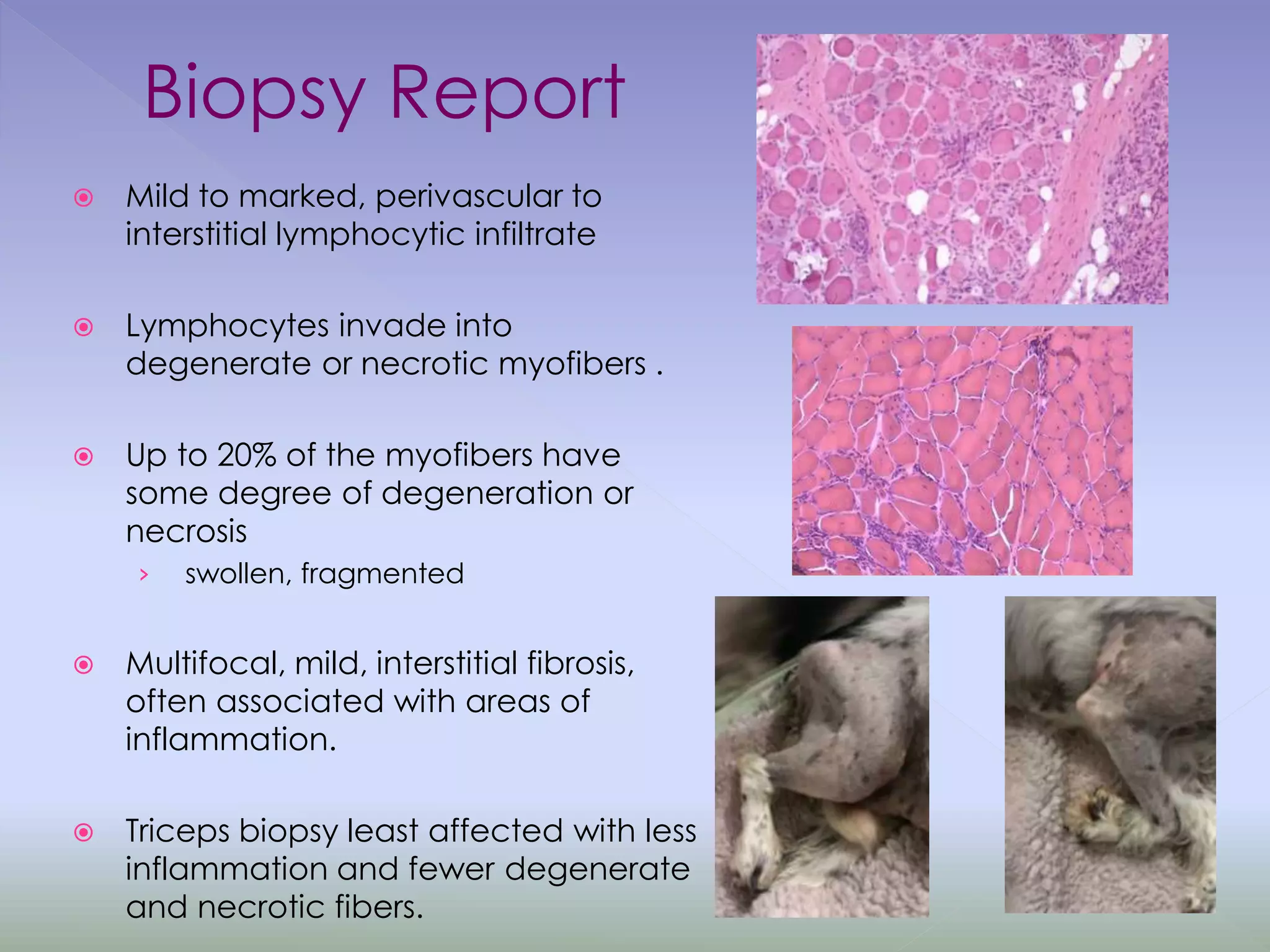
Bracken, an 11-year-old English Springer Spaniel, presented with a 5-week history of paraparesis, lethargy, and decreased appetite. Clinical examination revealed weakness in all limbs, especially the hind limbs. Diagnostic testing showed an elevated creatine kinase level and abnormal electromyography results. A small bladder mass and enlarged lymph node were also found. A muscle biopsy displayed lymphocytic infiltration and necrosis consistent with polymyositis. Bracken was diagnosed with immune-mediated polymyositis and started on immunosuppressive treatment and physical therapy. His condition is slowly improving.