Downloaded 679 times
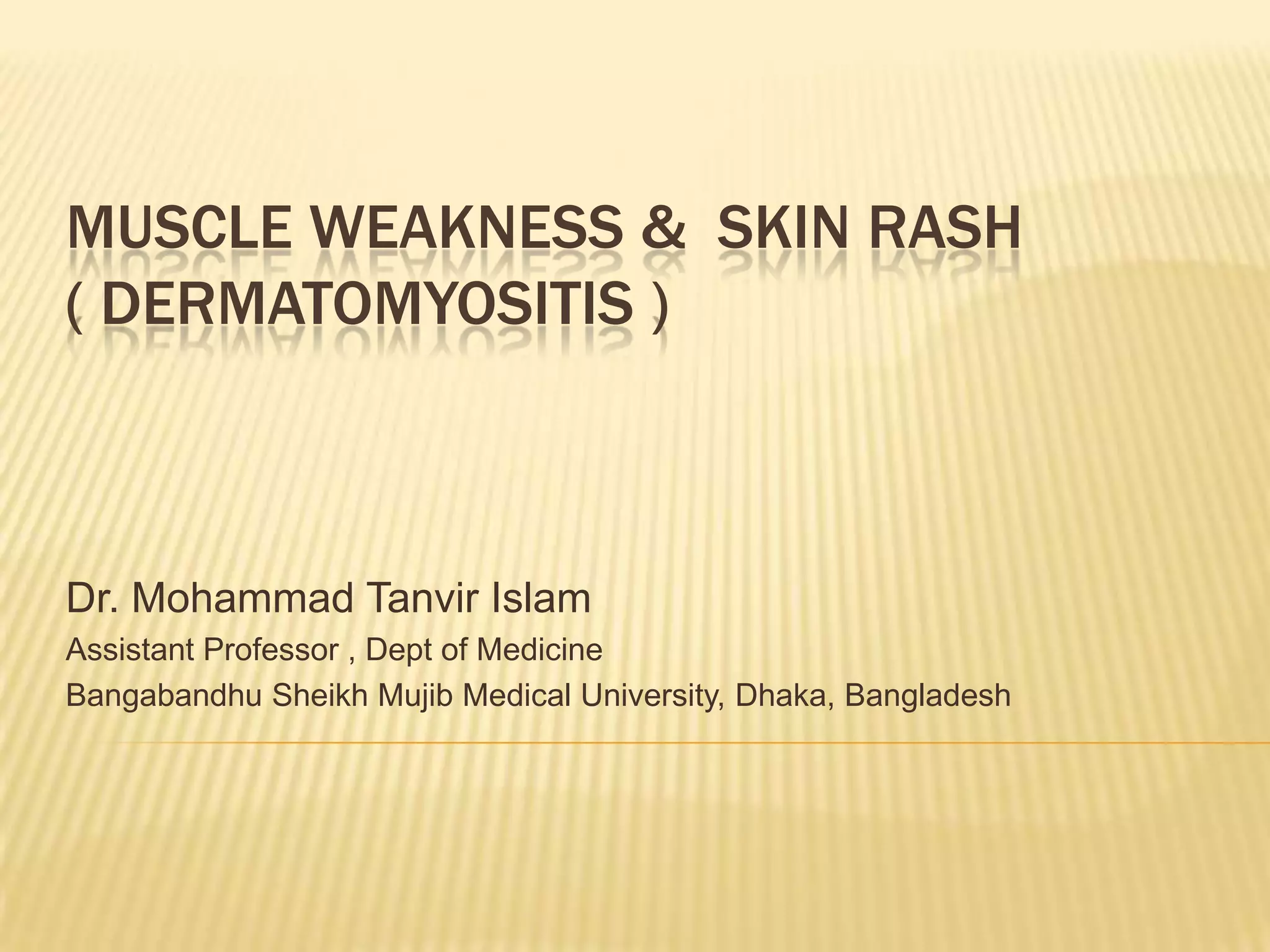
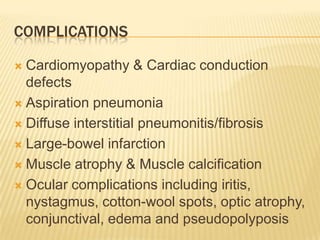
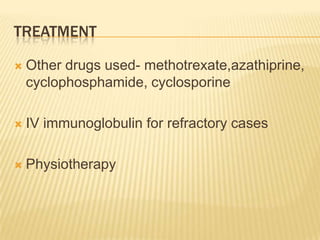
![CLASSIFICATION CRITERIA FOR POLYMYOSITIS
AND DERMATOMYOSITIS*
1. Skin lesions
Heliotrope: red-purple edematous erythema on the upper palpebra
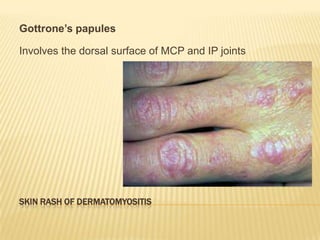
Gottron’s sign: red-purple keratotic, atrophic erythema or macules on the
extensor surface of finger joints
Erythema on the extensor surface of extremity joints, slight raised red-purple
erythema over elbows or knees
2. Proximal muscle weakness (upper or lower extremity and trunk)
3. Elevated serum creatine kinase or aldolase level
4. Muscle pain on grasping or spontaneous pain
5. Myogenic changes on electromyography (short-duration, polyphasic motor
unit potentials with spontaneous fibrillation potentials)
6. Positive anti-Jo-1 antibody test (histidyl-tRNA synthetase)
7. Nondestructive arthritis or arthralgias
8. Systemic inflammatory signs (temperature: more than 37°C [98.6°F] at axilla,
elevated serum C-reactive protein level or accelerated erythrocyte
sedimentation rate of more than 20 mm per hour by Westergren)
9. Pathologic findings compatible with inflammatory myositis (inflammatory
infiltration of skeletal evidence of active regeneration may be seen)](https://image.slidesharecdn.com/muscleweaknessrash-120531020648-phpapp02/85/Muscle-weakness-rash-Dermatomyositis-13-320.jpg)
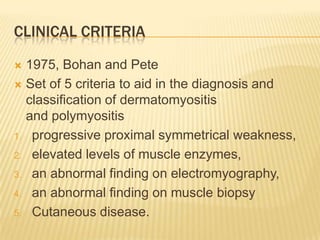
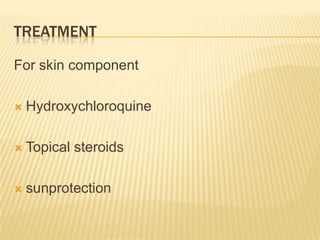
![SUBSETS OF MYOSITIS
Bohan and Peter suggested 5 subsets of myositis, as
follows :
Dermatomyositis
Polymyositis
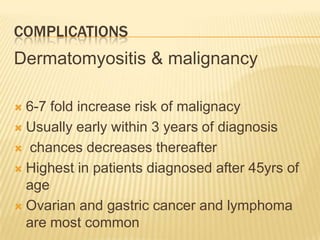
Myositis with malignancy
Childhood dermatomyositis/polymyositis
Myositis overlapping with another collagen-vascular
disorder
Others-
postmyopathic dermatomyositis
amyopathic dermatomyositis [ADM], or dermatomyositis
sine myositis](https://image.slidesharecdn.com/muscleweaknessrash-120531020648-phpapp02/85/Muscle-weakness-rash-Dermatomyositis-15-320.jpg)

This document discusses muscle weakness and skin rash (dermatomyositis). It provides information on the clinical presentation, causes, diagnostic criteria and classification, investigations, histopathological findings, treatment and prognosis of dermatomyositis. Key points include that dermatomyositis involves proximal muscle weakness and a skin rash. Diagnosis involves elevated muscle enzymes, electromyography, muscle biopsy and the presence of a skin rash. Treatment primarily involves oral steroids. Prognosis depends on factors like age, presence of malignancy and disease recalcitrance.










































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


















