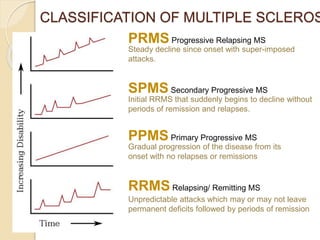
Multiple sclerosis is a chronic disease that damages the protective sheath surrounding nerve fibers in the brain and spinal cord. The immune system attacks this sheath, called myelin, which causes communication problems between the brain and body. The cause is unknown but likely involves genetic and environmental factors. Symptoms vary depending on the location of damage but can include numbness, vision problems, weakness, and impaired coordination. Diagnosis involves neurological exams, MRI images showing lesions in the brain and spine, and analysis of cerebrospinal fluid. While there is no cure, treatments aim to reduce frequency and severity of attacks and manage symptoms. Prognosis depends on the specific symptoms and disease progression in early years.



























































![Multiple Sclerosis[1]](https://cdn.slidesharecdn.com/ss_thumbnails/multiple-sclerosis1-1233826123956105-1-thumbnail.jpg?width=640&height=640&fit=bounds)





























![Multiple sclerosis- Sushila [Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/multiplesclerosis-sushilaautosaved-230522133935-4f68df92-thumbnail.jpg?width=640&height=640&fit=bounds)



































