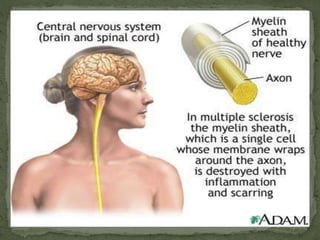
This document provides an overview of demyelinating diseases of the central nervous system, with a focus on multiple sclerosis. It discusses the etiology, pathogenesis, clinical features, diagnosis, treatment and management of multiple sclerosis. Key points include: MS results from an autoimmune attack on the myelin sheath surrounding nerves in the brain and spinal cord; diagnosis involves evidence of lesions disseminated in space and time via MRI or other tests; and treatments include steroids for acute attacks and disease-modifying drugs such as interferons to reduce relapse rates long-term.






























































































![Myelin Oligodendrocyte Glycoprotein (MOG) Antibody Disease [MOG-AD]](https://cdn.slidesharecdn.com/ss_thumbnails/myelinoligodendrocyteglycoproteinmogantibodydisease0920-200920055159-thumbnail.jpg?width=640&height=640&fit=bounds)










































