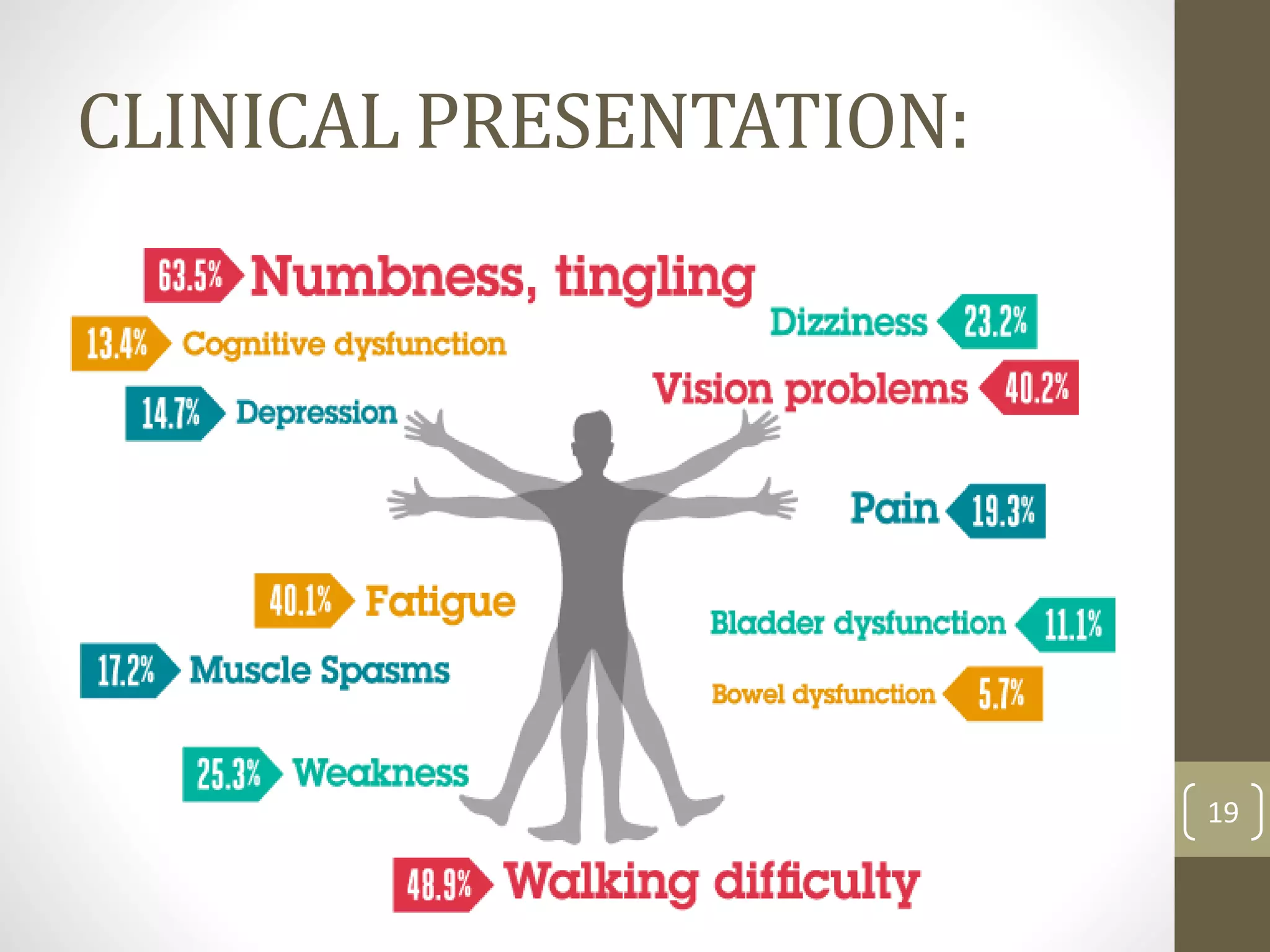
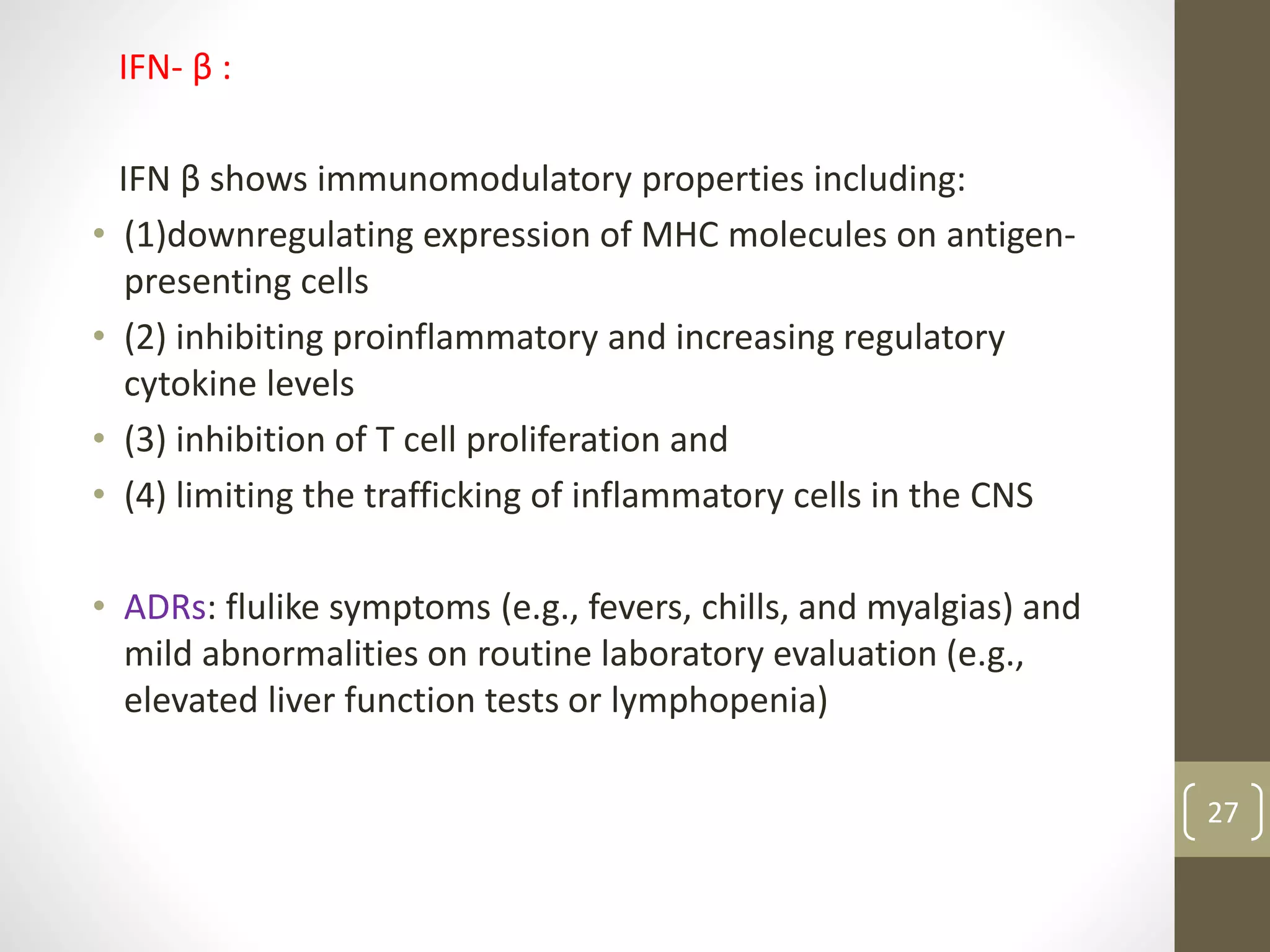
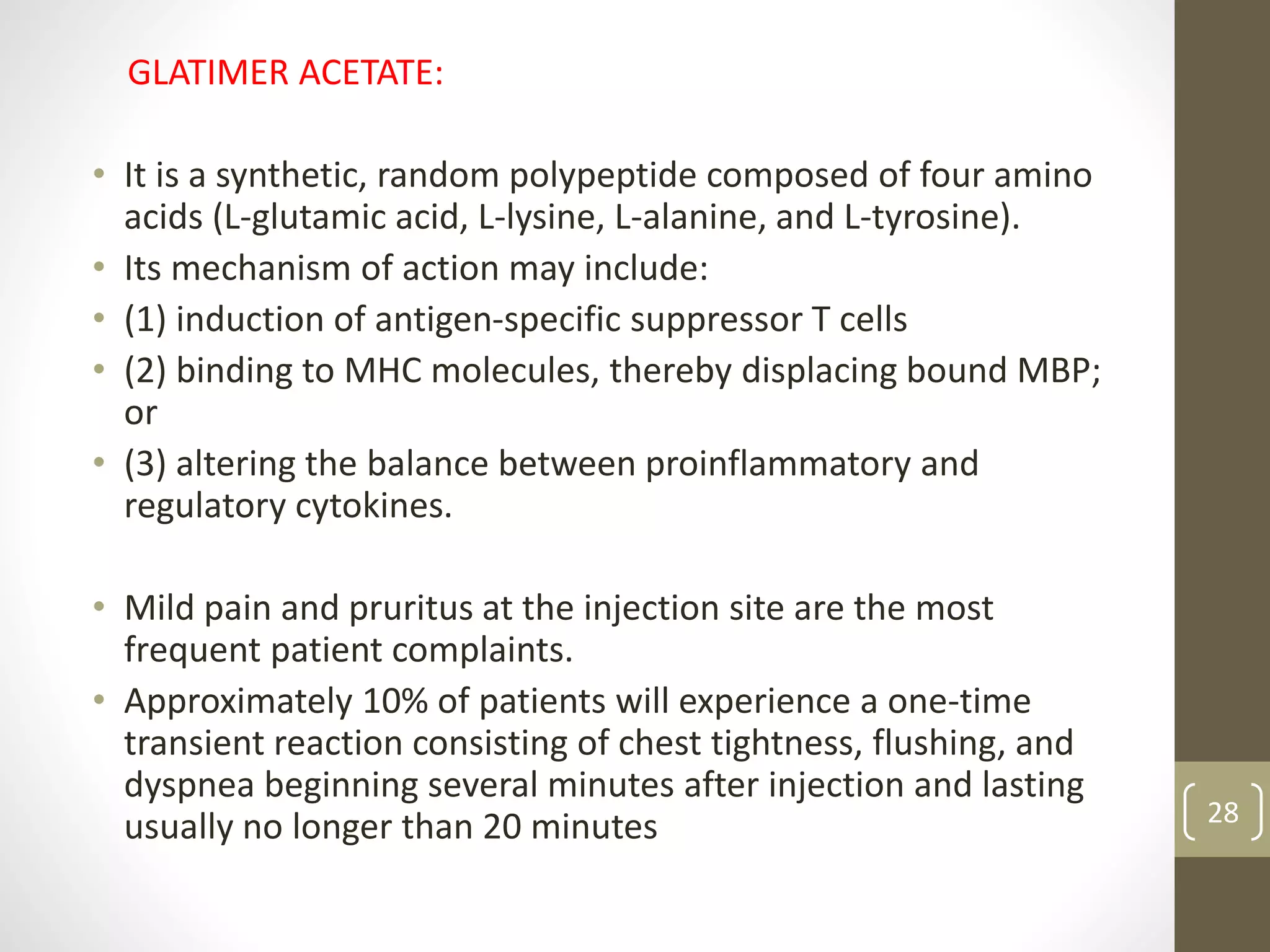
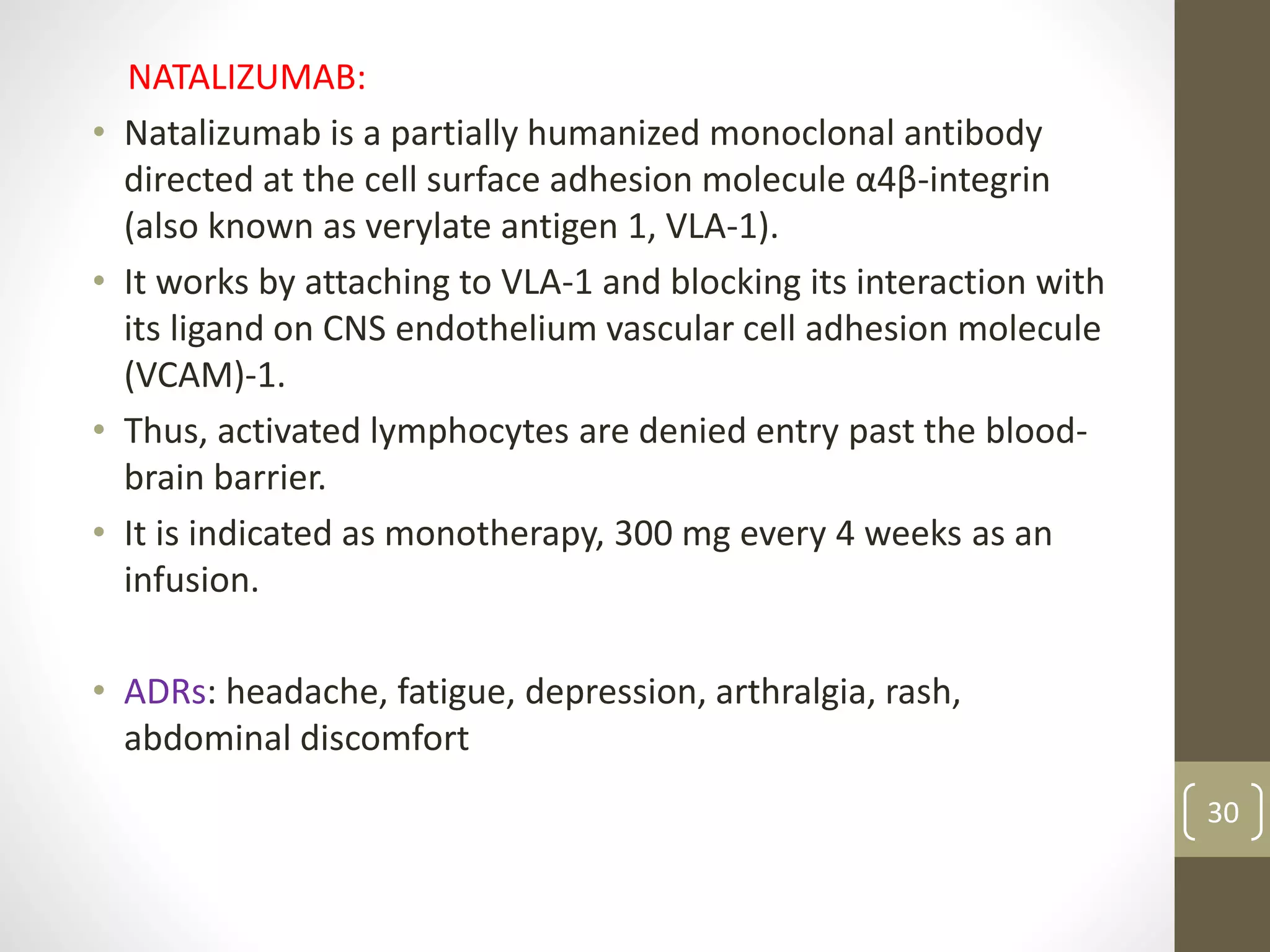
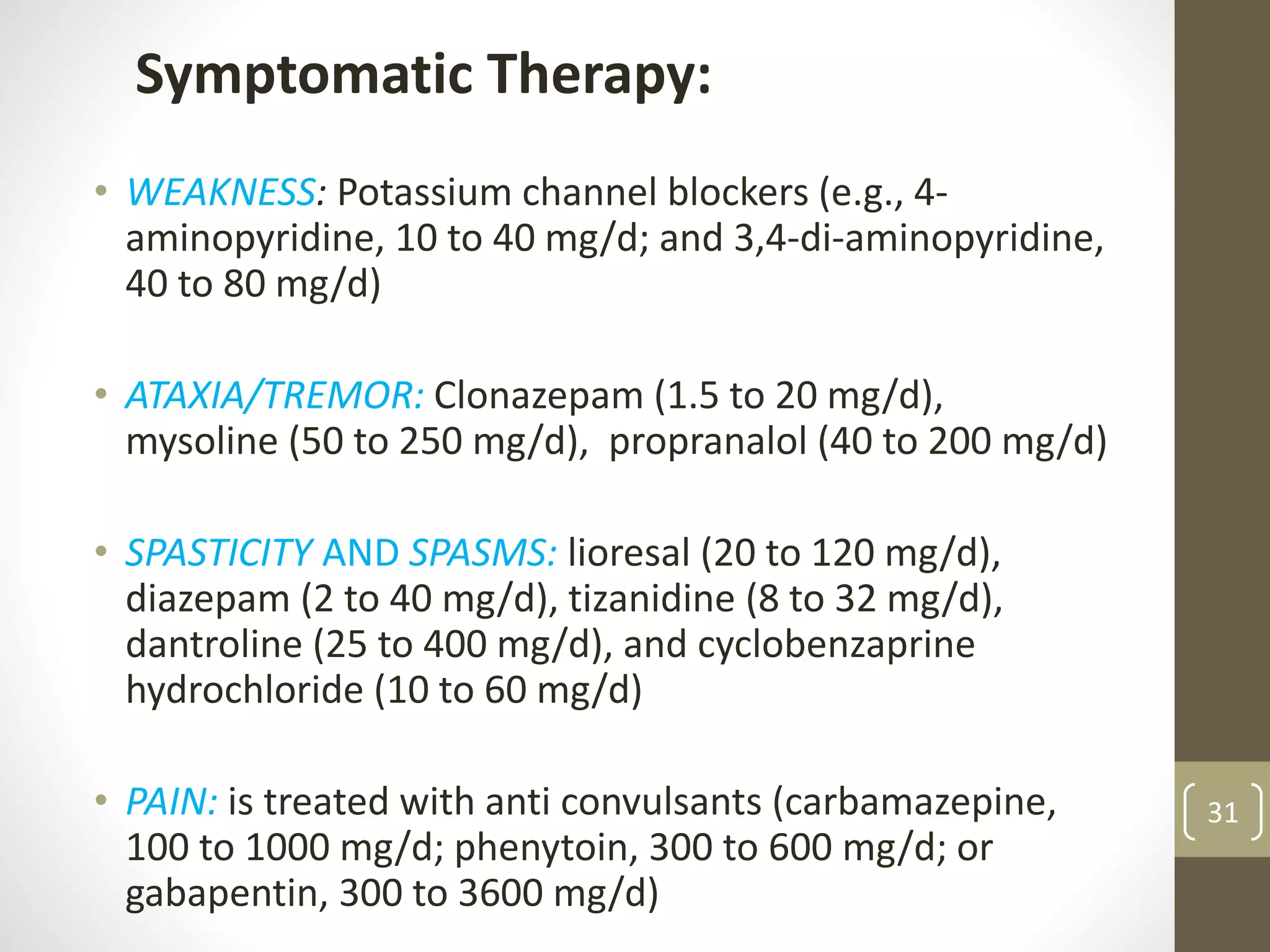
This document provides information on Multiple Sclerosis (MS), including its epidemiology, etiology, clinical presentation, diagnostic tests, disease course, and treatment options. MS is an immune-mediated disease that attacks the central nervous system, destroying myelin and axons. Common symptoms include visual changes, numbness, weakness, and balance issues. Diagnosis involves MRI, lumbar puncture for cerebrospinal fluid analysis, and evoked potentials testing. The disease course varies between relapsing-remitting, primary progressive, and secondary progressive forms. Treatment focuses on reducing inflammation and disability through medications like interferon beta, glatiramer acetate, and natalizumab, as well as managing symptoms with drugs for pain,





















































![Multiple Sclerosis[1]](https://cdn.slidesharecdn.com/ss_thumbnails/multiple-sclerosis1-1233826123956105-1-thumbnail.jpg?width=640&height=640&fit=bounds)













![Multiple sclerosis- Sushila [Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/multiplesclerosis-sushilaautosaved-230522133935-4f68df92-thumbnail.jpg?width=640&height=640&fit=bounds)













































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)

