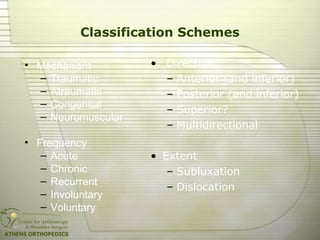
This document discusses multi-directional shoulder instability (MDI). MDI is characterized by subluxations or dislocations in at least two directions, usually anteriorly, posteriorly, or inferiorly. It is commonly seen in overhead athletes and is associated with capsular laxity. Clinical examination reveals laxity and translation in multiple directions. Treatment involves strengthening dynamic stabilizers through physical therapy initially, with surgery such as arthroscopic capsular plication considered if conservative measures fail. Post-operative rehabilitation is important for successful outcomes. Long-term, over half of untreated MDI patients experience pain and instability.


![MDI Surgical Treatment
The goal is "addressing the capsular
laxity and redundancy to restore
anatomic capsuloligamentous tension
without overconstraining the shoulder."
[Caprise and Sekiya, 2006]
www.shoulder.gr](https://image.slidesharecdn.com/nkyy5rmjsveeupwzeby7-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100657/85/Multidirectional-shoulder-instability-35-320.jpg)

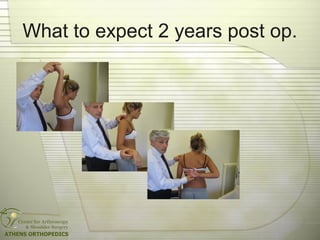
![What to expect
• Painless shoulder
• Full ROM
• No atrophies
• Return to the same sport level
Rowe scores:
78% excellent / good [Snyder, 2001]
75% excellent / good [Wolf, 1999]
88% excellent / good [Treacy, 2002]
www.shoulder.gr](https://image.slidesharecdn.com/nkyy5rmjsveeupwzeby7-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100657/85/Multidirectional-shoulder-instability-41-320.jpg)




![Natural History Of MDI
After 8 years:
• 48.7% pain 46.1% instability
• Mod. Rowe/Zarris:
• 13.8% excellent
• 33% good
• 52.7% poor
[Misamore, JSES 2005]
www.shoulder.gr](https://image.slidesharecdn.com/nkyy5rmjsveeupwzeby7-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100657/85/Multidirectional-shoulder-instability-50-320.jpg)























































































