Downloaded 355 times
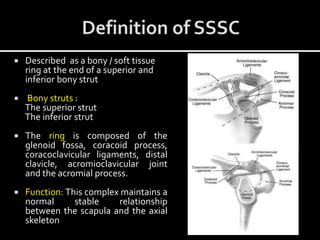
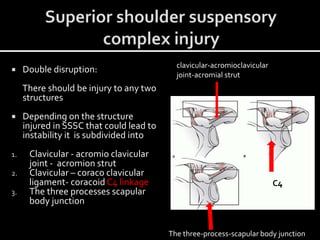

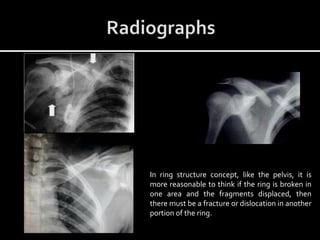
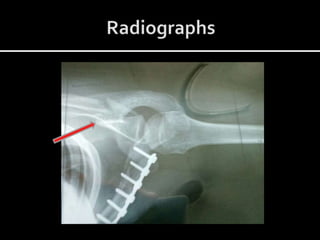
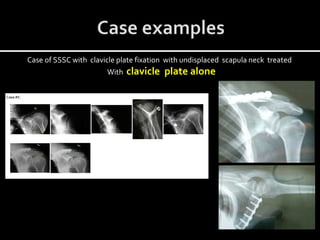
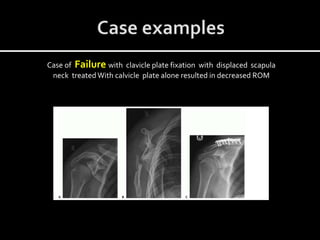
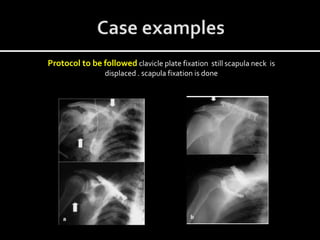
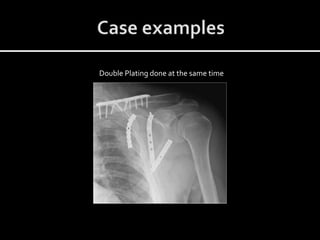
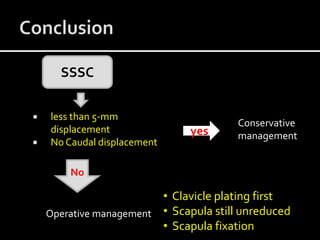


This document discusses zonal CME conducted at GSLMC on the superior shoulder suspensory complex (SSSC). It defines the SSSC as a bony and soft tissue ring structure that maintains the stable relationship between the scapula and axial skeleton. Injuries to two structures in the SSSC can cause instability known as the "floating shoulder". Treatment depends on the amount of displacement, with conservative management used for displacements under 5mm and no caudal displacement of the glenoid. Surgical stabilization is recommended for larger displacements or malalignment.





































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










