Downloaded 43 times

![MDI
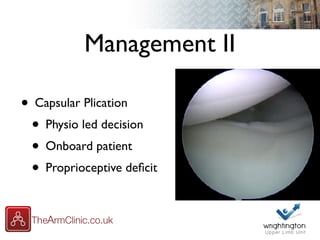
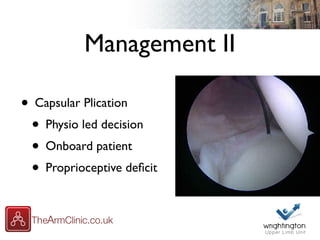
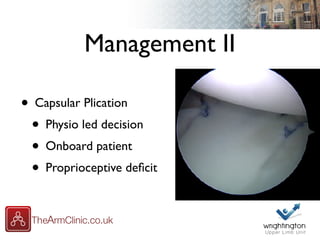
• Definition “MultiDirectional Instability”
• Shoulder instability in patients who have
generalised ligamentous laxity [Web Dictionary]
• Abnormal exclusion of the humeral head
on the glenoid in ALL directions [Neer]
• Instability in TWO directions [1,2,3,4]
• Instability in THREE directions [5,6,7]](https://image.slidesharecdn.com/macatraumaticinstabiliitya2-170405132119/85/Atraumatic-Shoulder-Instability-16-320.jpg)




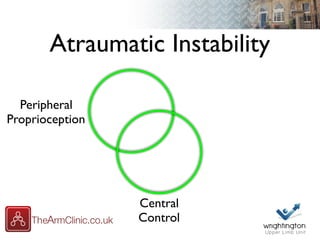
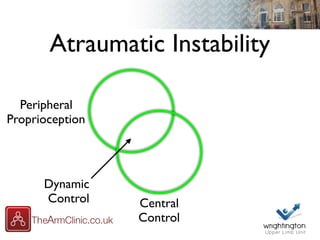




The document discusses atraumatic shoulder instability, focusing on multidirectional instability (MDI) and its classification, causes, and management strategies. It reviews the biomechanics involved, dynamic control factors, and assessment techniques for patients experiencing instability, emphasizing the importance of understanding patient histories and individual symptoms. Furthermore, it outlines treatment approaches, including physiotherapy and surgical options such as capsular plication.



















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



