Downloaded 460 times












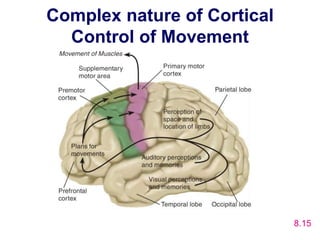

























































The motor system consists of upper motor neurons originating in the motor cortex and lower motor neurons originating in the spinal cord. The motor cortex is located in the frontal lobe and contains a somatotopic map called the motor homunculus. Primary motor areas directly control movement while secondary areas like the premotor and supplementary motor areas plan movements. The corticospinal tract originates from the primary motor cortex and controls voluntary movement. Extrapyramidal tracts like the reticulospinal and vestibulospinal tracts modify motor function. Lesions of the upper or lower motor neurons result in different clinical presentations like spasticity, flaccidity, weakness and abnormal reflexes. Common neurological diseases that affect the motor system include





















































































