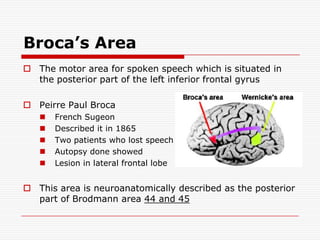
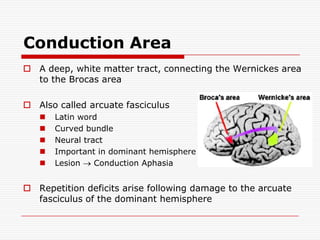
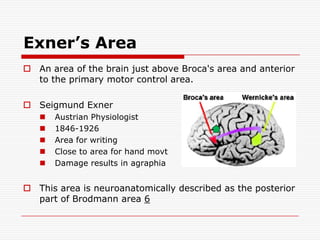
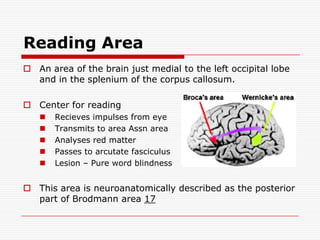
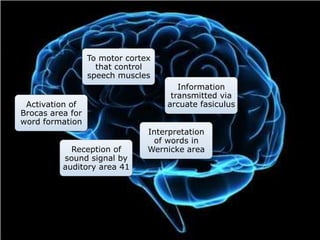
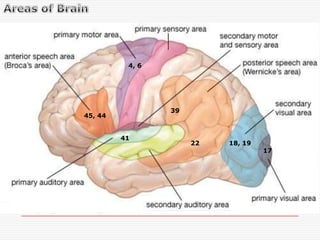
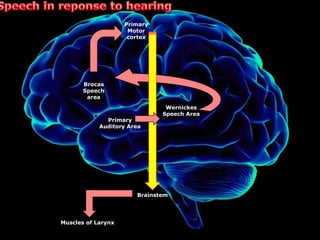
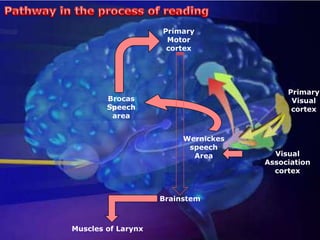
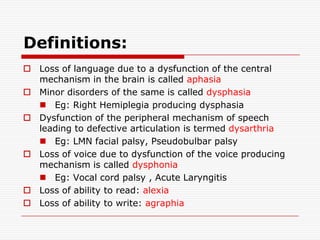
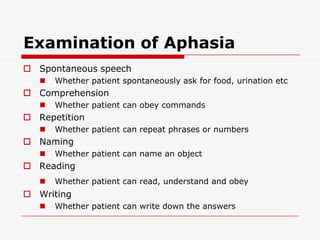
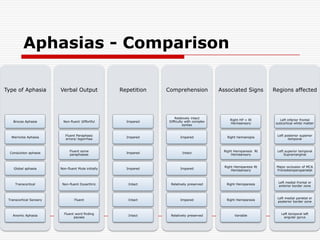


The document discusses the detailed anatomy and mechanisms of speech, language, and aphasia, emphasizing the roles of various brain areas such as Wernicke's and Broca's areas. It defines aphasia as a loss of language due to brain dysfunction, explores different types of aphasia (e.g., Broca's, Wernicke's, conduction aphasia), and outlines methods for testing language skills. Additionally, it highlights related disorders, including apraxia and agnosia, affecting motor skills and sensory recognition, respectively.























































































