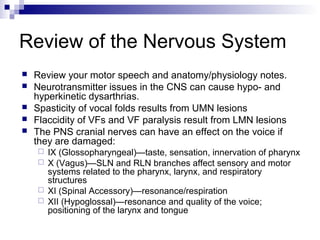
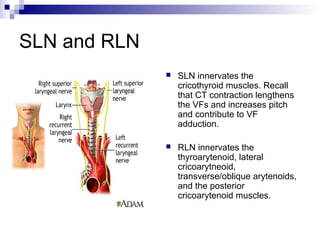
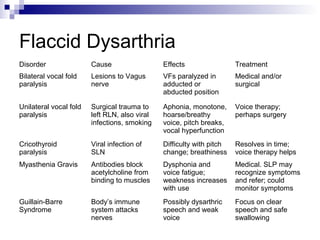
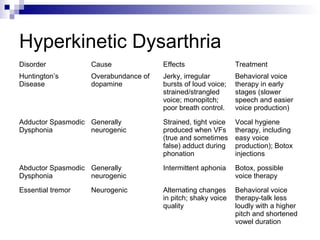
This document discusses neurogenic voice disorders. It reviews the anatomy and physiology of the nervous system related to voice production. Damage to lower motor neurons can cause flaccidity of the vocal folds, while upper motor neuron lesions can cause spasticity. Various cranial nerves like the vagus, accessory, and hypoglossal nerves also affect voice. Lesions of the recurrent laryngeal nerve or superior laryngeal nerve impact vocal fold function. Different types of dysarthrias are then outlined, including their causes, symptoms, and treatment approaches.


























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)










