Downloaded 146 times

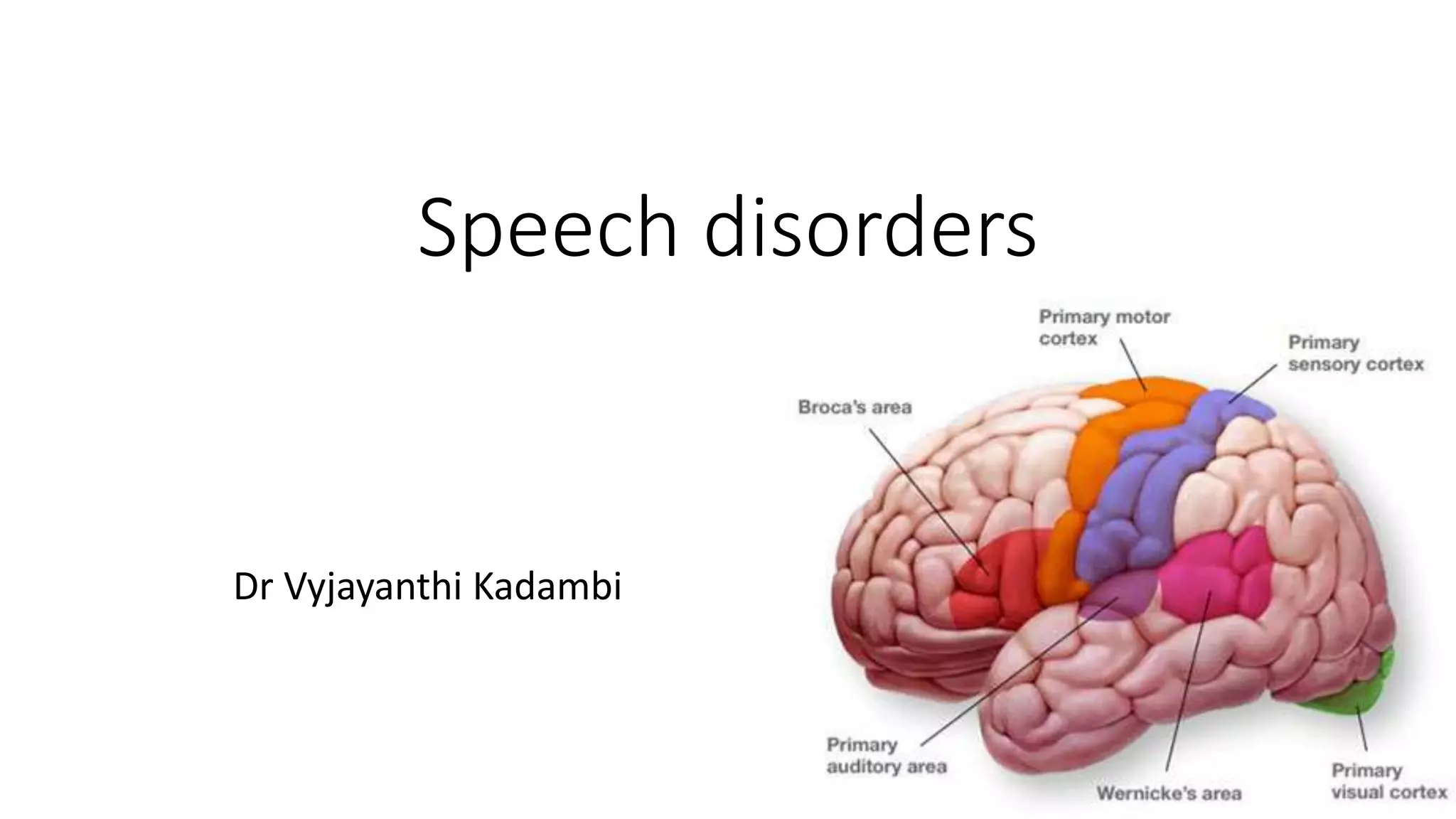

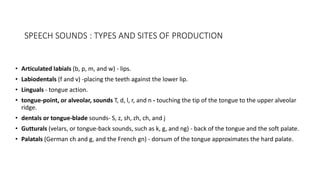
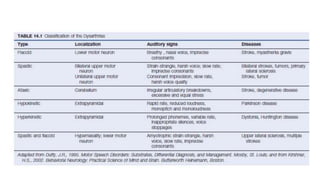
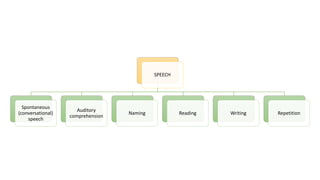
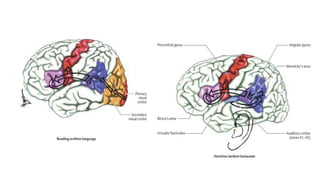

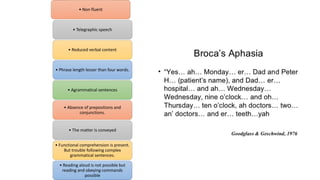
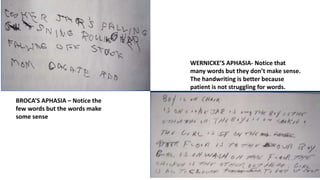
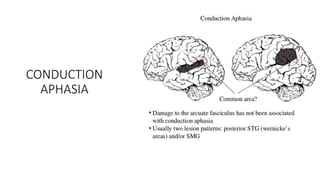

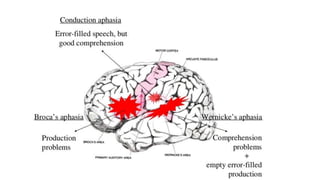




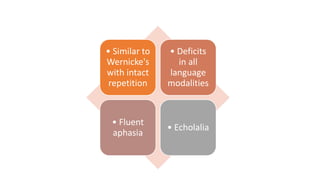

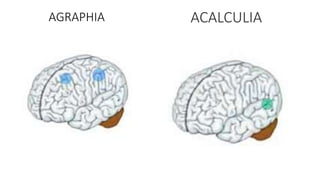
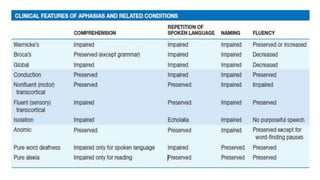
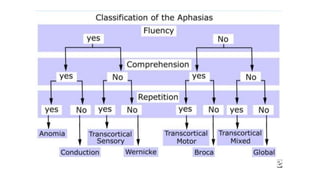


This document discusses speech disorders and their classification. It covers the anatomy and physiology of speech production, different types of speech disorders like aphasia and dysarthria, and their causes and management. Aphasia refers to language impairment due to brain damage and can cause deficits in speaking, comprehension, reading and writing. Dysarthria is defective articulation due to neurological problems, while language functions remain intact. Speech disorders are classified as disorders of language like aphasia or disorders of articulation/voice production.



































































