This document provides an overview of auditory middle latency response (AMLR) testing, including:
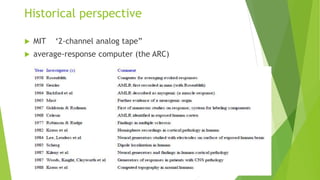
1. A brief history and the development of AMLR from early clinical studies to its current uses for evaluating auditory thresholds and cortical function.
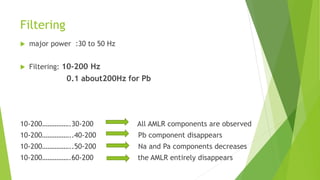
2. Details on stimulus parameters like rate, intensity and transducer type that influence AMLR waveforms.
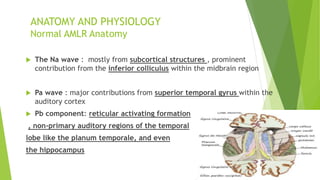
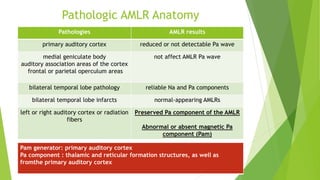
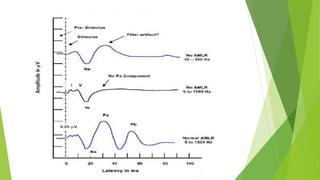
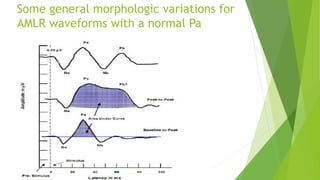
3. Descriptions of the anatomy and physiology underlying AMLR waves like Na, Pa and Pb, and how various pathologies can affect the waves.
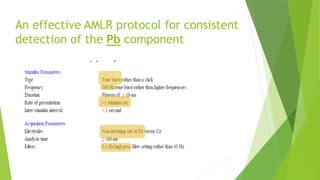
4. Guidelines for acquisition parameters like electrodes, filtering and analysis windows to reliably detect AMLR components.
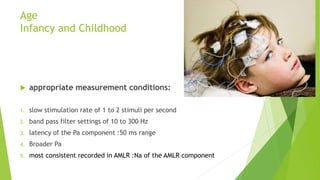
5. Factors like age, attention, drugs and medical