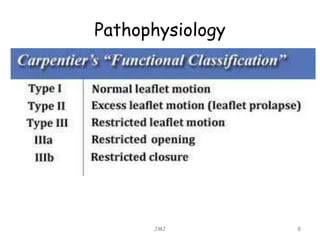
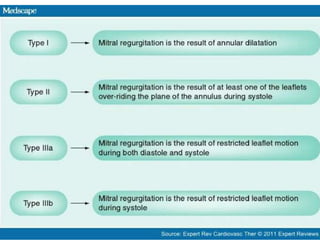
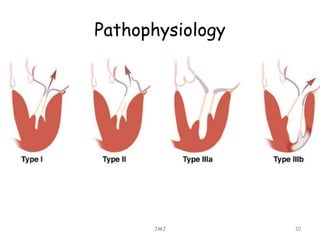
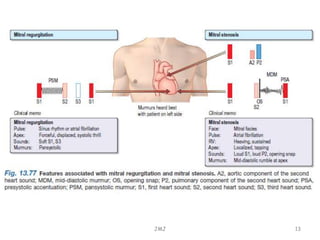

The document discusses mitral regurgitation, detailing its causes such as degenerative disease, ischemic heart disease, and infectious endocarditis. It explains the pathophysiology, symptoms, signs, and investigation methods including echocardiograms and electrocardiograms. Treatment options are mentioned, focusing on prophylaxis against endocarditis and options for surgical intervention if progressive cardiac enlargement is detected.





























































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)













