
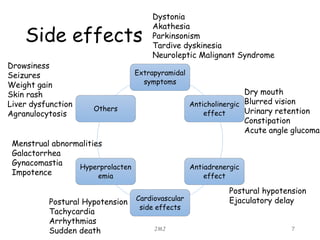


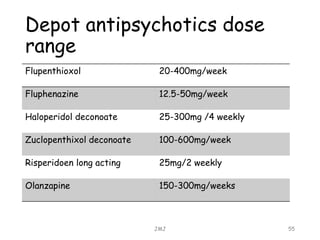

The document provides an overview of antipsychotics, categorizing them into first and second generations, along with specific medications and their actions, indications, side effects, and management of those side effects. It details dosing instructions, cautions, and monitoring requirements, particularly for clozapine, as well as intramuscular and depot formulations for rapid tranquilization. Additionally, it highlights the metabolic risks associated with antipsychotic use and the importance of regular monitoring to mitigate these risks.























































































