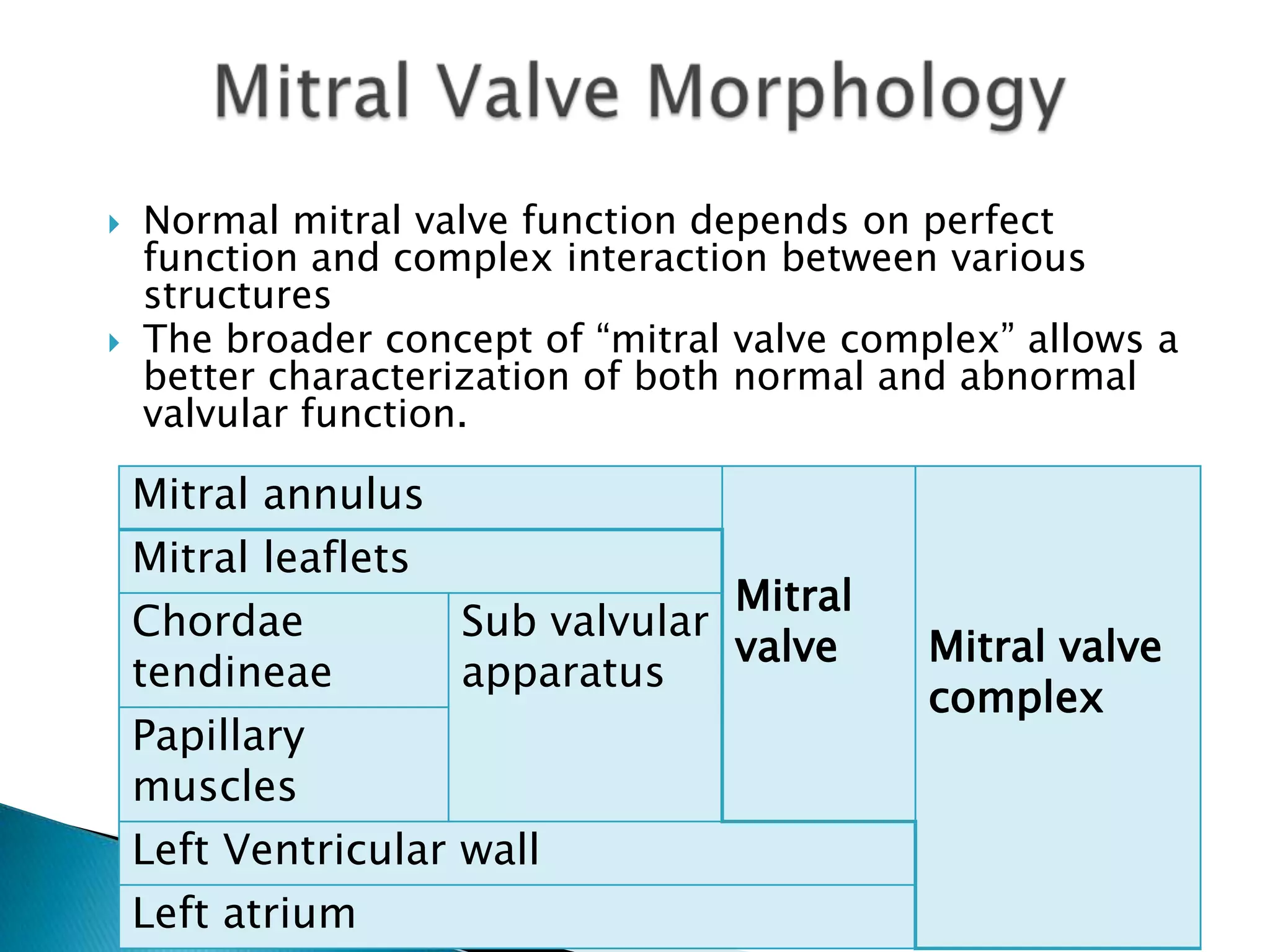
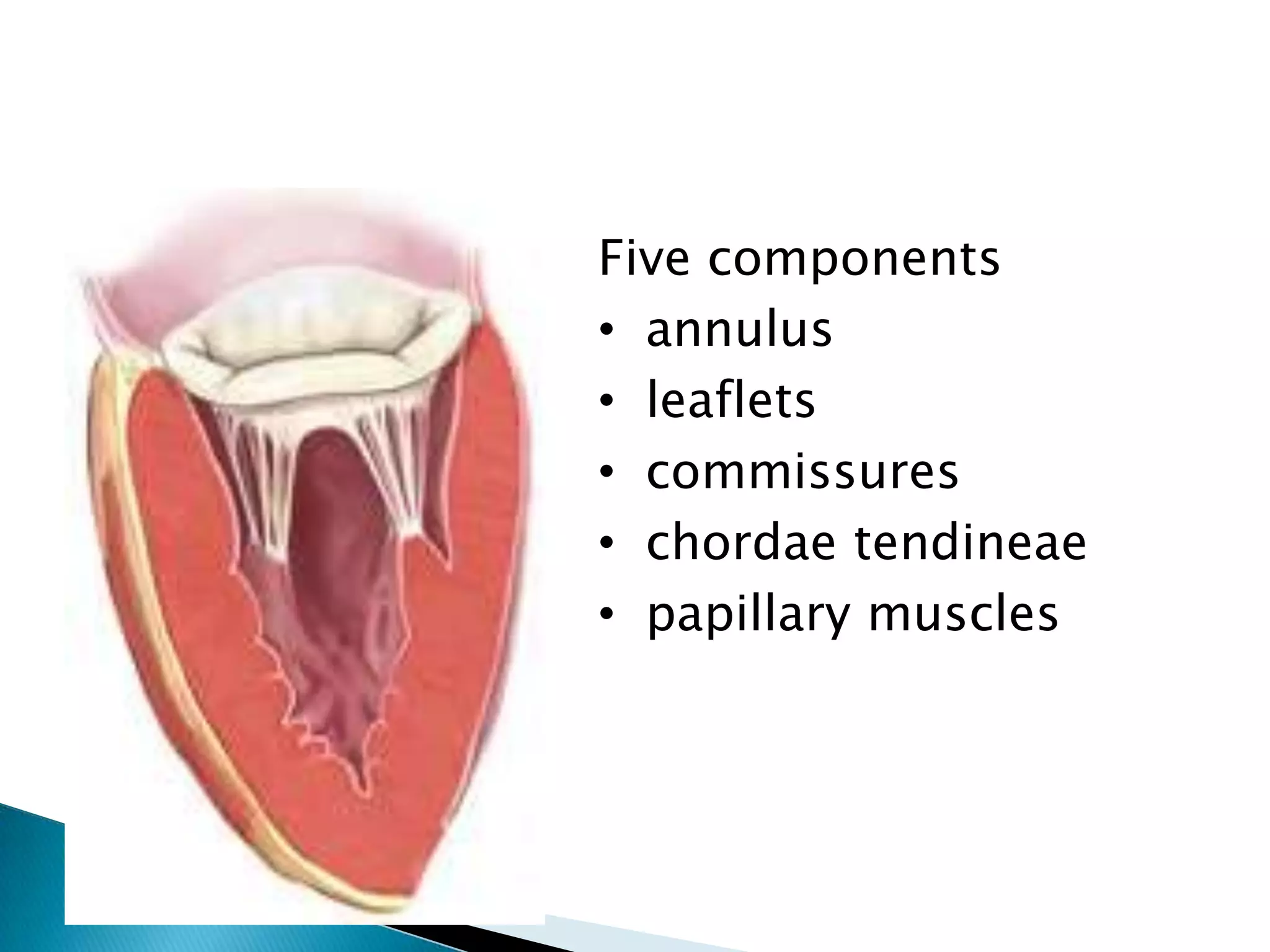
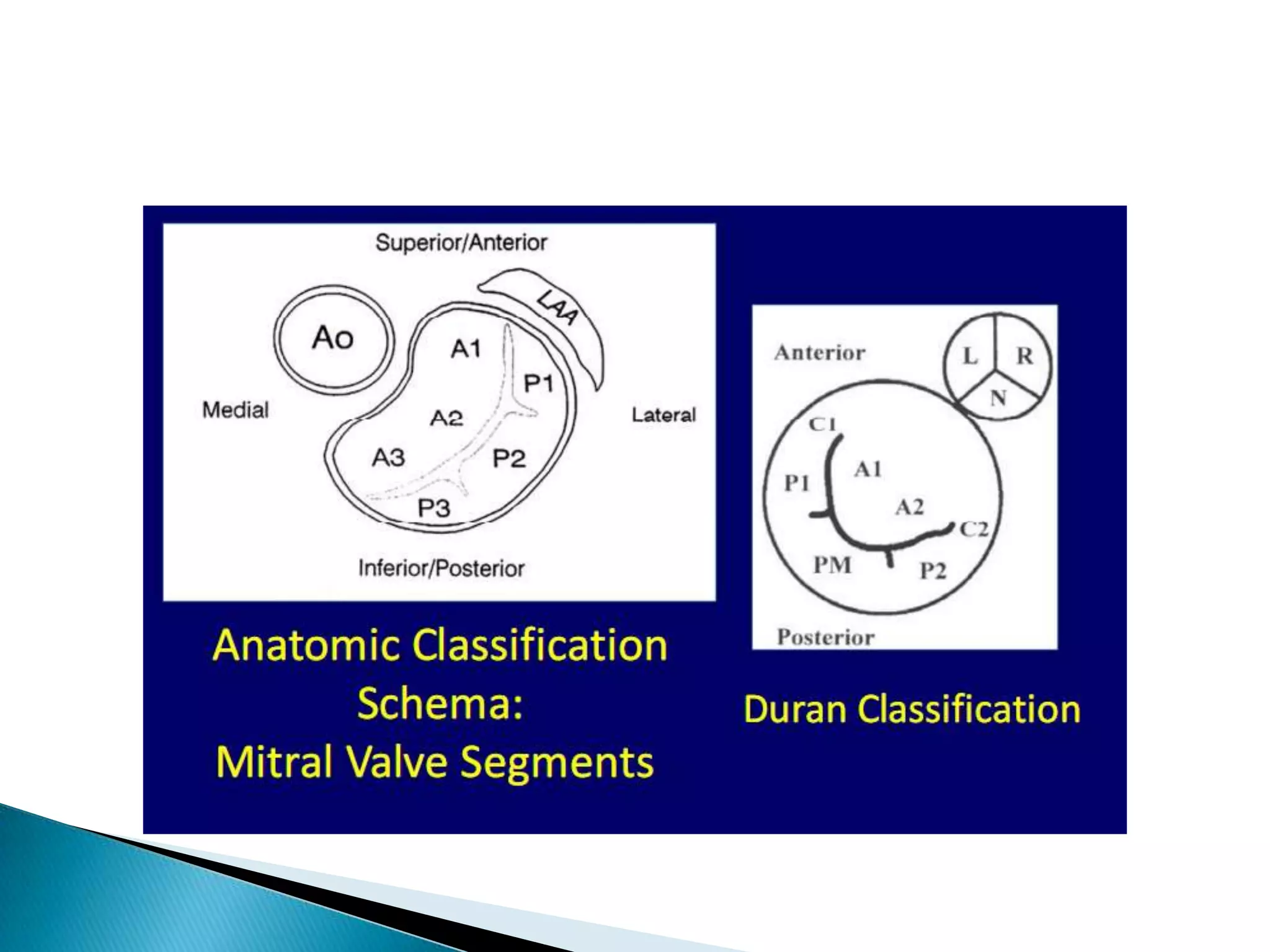
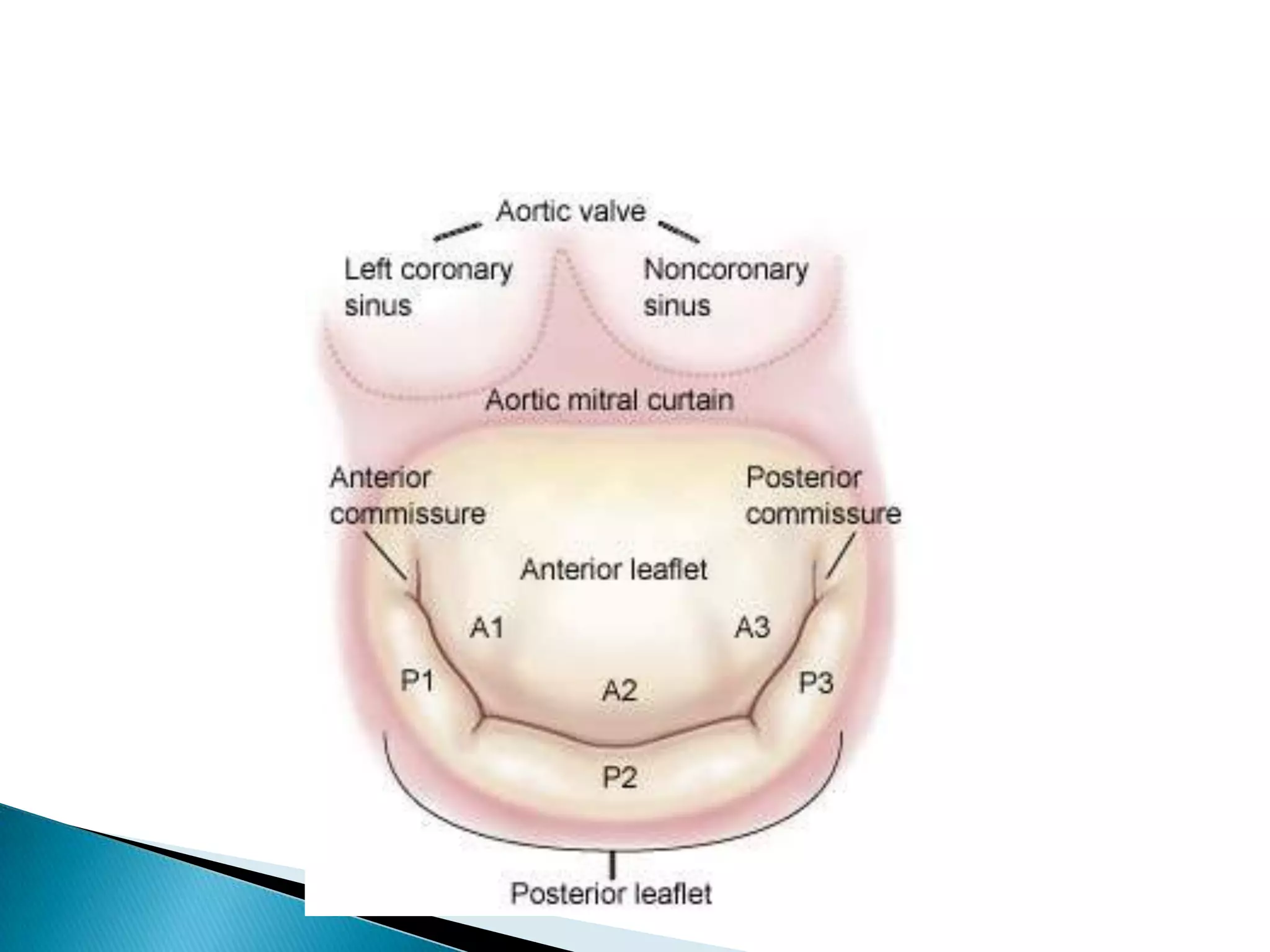
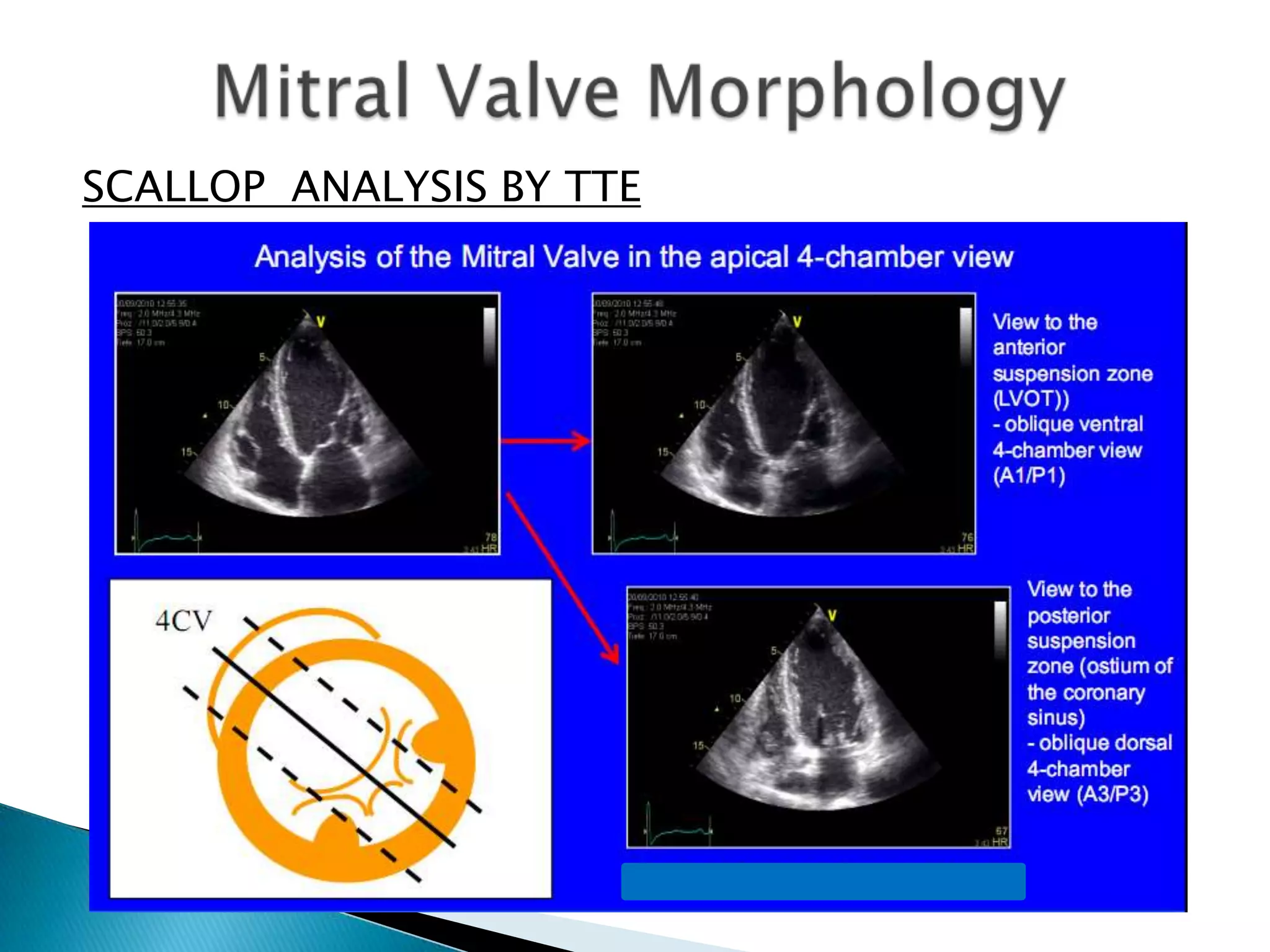
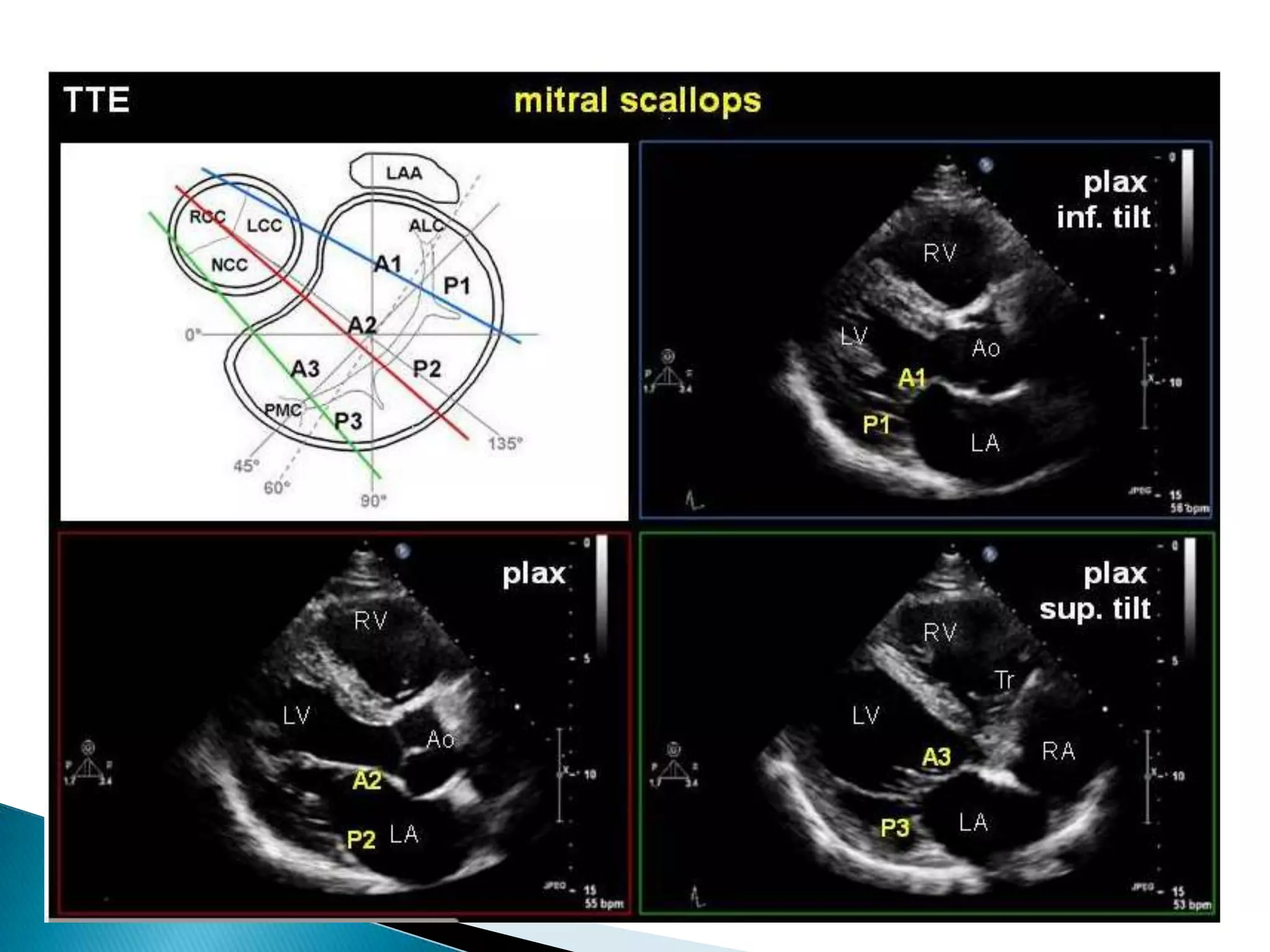
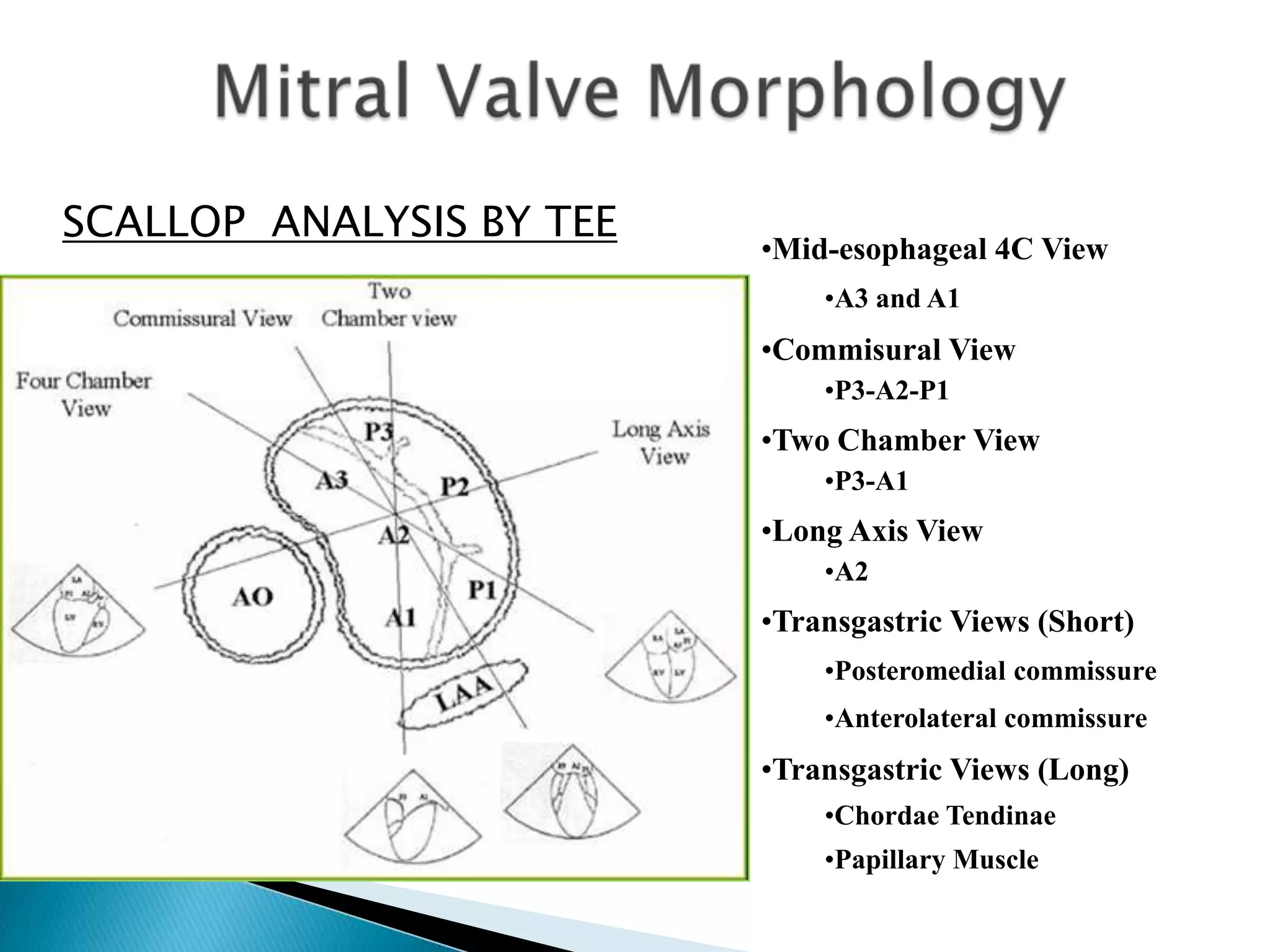
The document discusses the anatomy and function of the mitral valve complex. It notes that the mitral valve has a triple function regulating blood flow between the left atrium and ventricle. The mitral valve complex relies on normal morphology and function of the annulus, leaflets, chordae tendineae, papillary muscles, and left ventricle. Echocardiography is useful for evaluating each of these structures and identifying abnormalities that can cause mitral dysfunction. Detailed assessment of the leaflet segments, called scallops, aids in characterizing valvular lesions.





















































































![Mitral_Valve_Anatomy_Surgical_Perspective[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/mitralvalveanatomysurgicalperspective1-250701160336-9898ca79-thumbnail.jpg?width=640&height=640&fit=bounds)






























