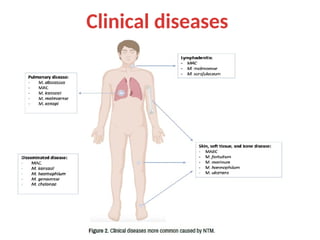
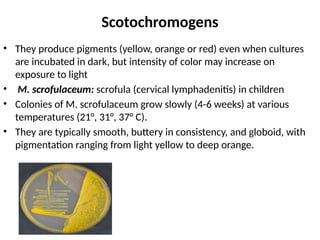
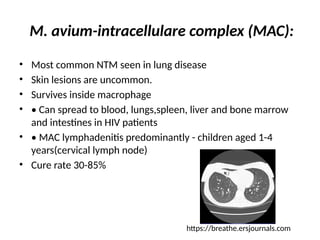
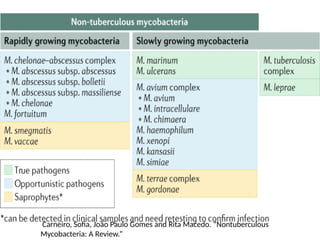
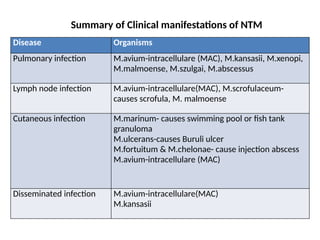
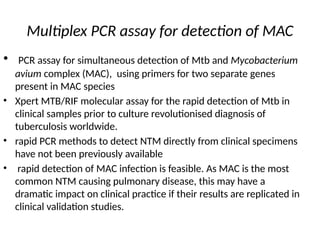
Nontuberculous mycobacteria (NTM) are environmental organisms that do not cause tuberculosis and are often opportunistic pathogens linked to human infections. They include various species associated with clinical diseases such as pulmonary infections, lymph node infections, and skin diseases, affecting primarily immunocompromised individuals. Diagnosis involves specific laboratory tests and treatments typically include multidrug therapy due to rising drug resistance.





![[Micro] mycobacterium tuberculosis](https://cdn.slidesharecdn.com/ss_thumbnails/knwspassdmixhofx5ycy-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190755-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
































![[Micro] atypical mycobacterium](https://cdn.slidesharecdn.com/ss_thumbnails/7d5djanirg26boloifek-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190753-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
















































