Downloaded 226 times
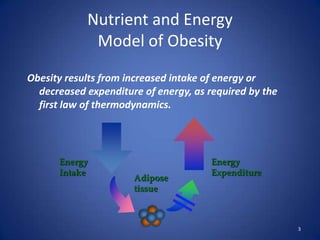

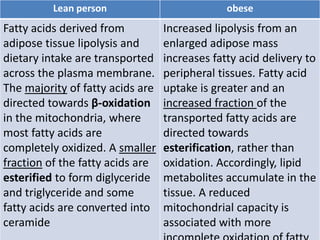
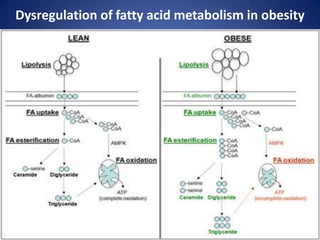




Metabolic abnormalities in obesity are caused by an imbalance between energy intake and expenditure over time. There are three main components of total energy expenditure - resting energy expenditure, the energy expended during physical activity, and the thermic effect of food. In obesity, resting energy expenditure is increased due to more adipose tissue, but the thermic effect of food is reduced. Adipose tissue stores triglycerides and also functions as an endocrine organ secreting hormones that influence metabolism. Dysregulation of lipid metabolism and adipokine secretion in obesity can lead to medical complications.








































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)










