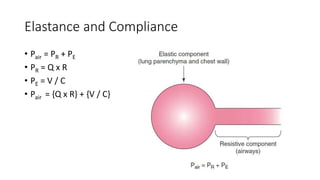
The document discusses monitoring respiratory mechanics during mechanical ventilation. It describes the resistive and elastic components of the respiratory system and how peak pressure, plateau pressure, compliance, and elastance are measured and affected. Peak pressure is the maximum pressure achieved in a breath and is impacted by resistance, flow, volume, and elastance. Plateau pressure measures lung parenchymal properties at a given volume. Compliance is the change in volume per unit change in pressure and can be measured statically or dynamically.