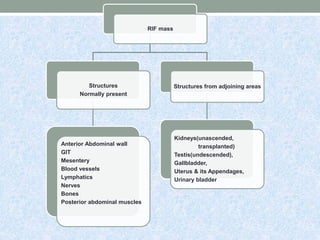
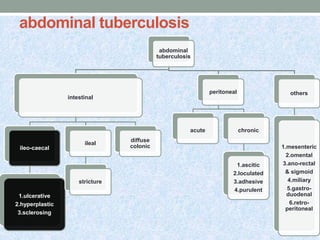
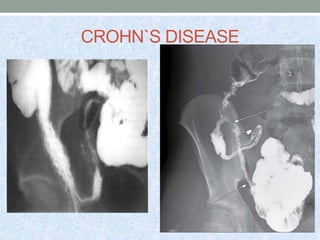
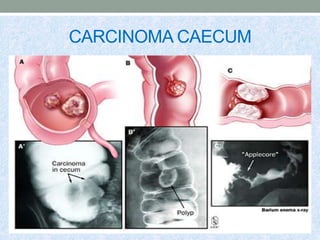
1. The document discusses various potential causes of a mass in the right iliac fossa, including appendicitis, appendicular abscess, carcinoid tumors of the appendix, mucoceles, adenocarcinoma, tuberculosis, Crohn's disease, carcinoma of the caecum, actinomycosis, amoebiasis, mesenteric cysts, intussusception, iliopsoas abscess, retroperitoneal tumors, aneurysms, and more rare causes.
2. Diagnostic tools mentioned include ultrasound, CT, colonoscopy, and biopsy. Treatment depends on the underlying cause but may include antibiotics, surgery, chemotherapy, and ATT.
3

























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)















