Downloaded 733 times

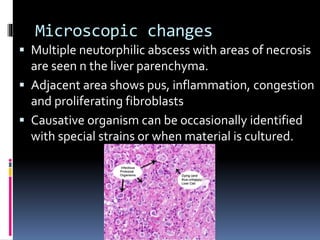
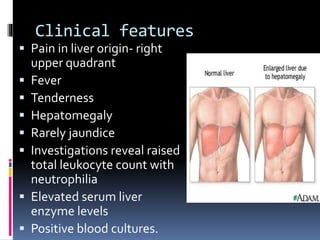

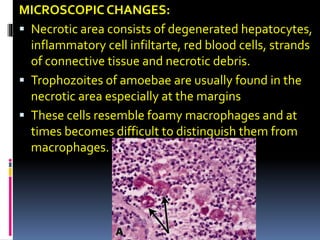
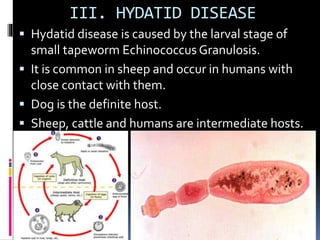


This document discusses different types of liver abscesses including their etiology, morphology, clinical features, and complications. Pyogenic liver abscesses are most commonly of bacterial origin such as E. coli. Amoebic liver abscesses are caused by the parasite Entamoeba histolytica and are more common in developing countries. Hydatid disease is caused by the larval stage of the tapeworm Echinococcus granulosus and presents as slow-growing cysts in the liver that can rupture and spread to other organs. Diagnosis involves blood tests, imaging, and biopsy of the abscess.













































































