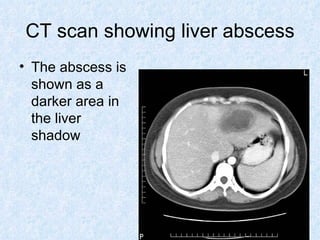
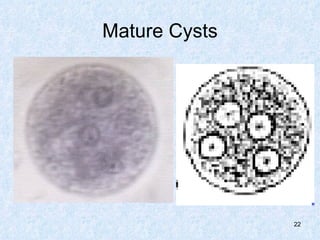
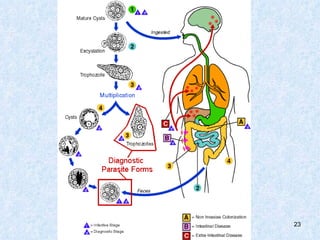
Liver abscesses are usually caused by bacteria, parasites or fungi entering through the biliary tract or portal vein. The most common type is a pyogenic abscess in the right lobe of the liver. Risk factors include chronic alcoholism. Entamoeba histolytica, the cause of amebic dysentery, can spread from the colon to the liver and cause an amoebic abscess. Symptoms include fever, right upper quadrant pain and tenderness. Diagnosis involves blood tests and imaging scans like ultrasound, CT or MRI. Treatment is with antibiotics and sometimes drainage of the abscess.