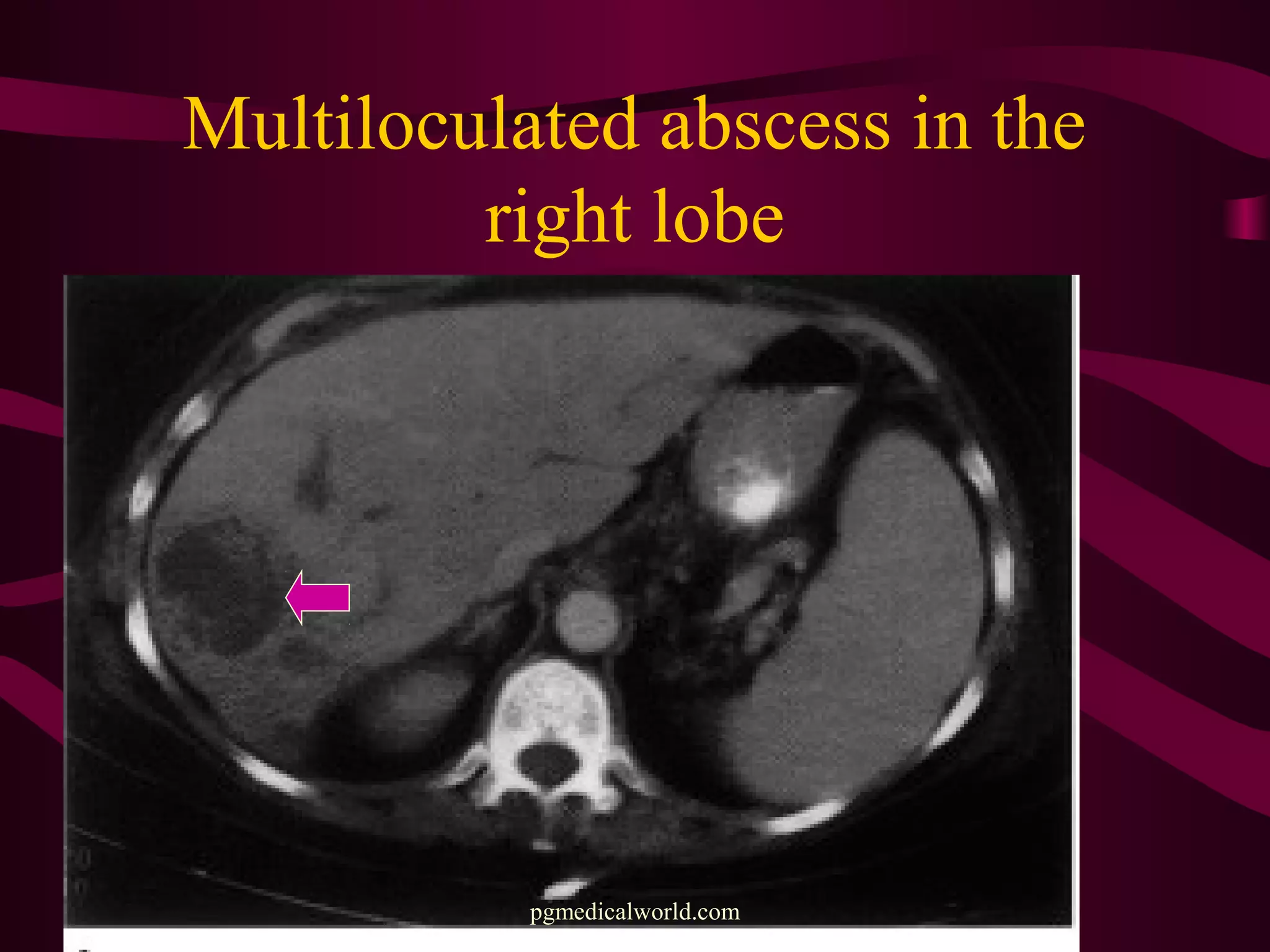
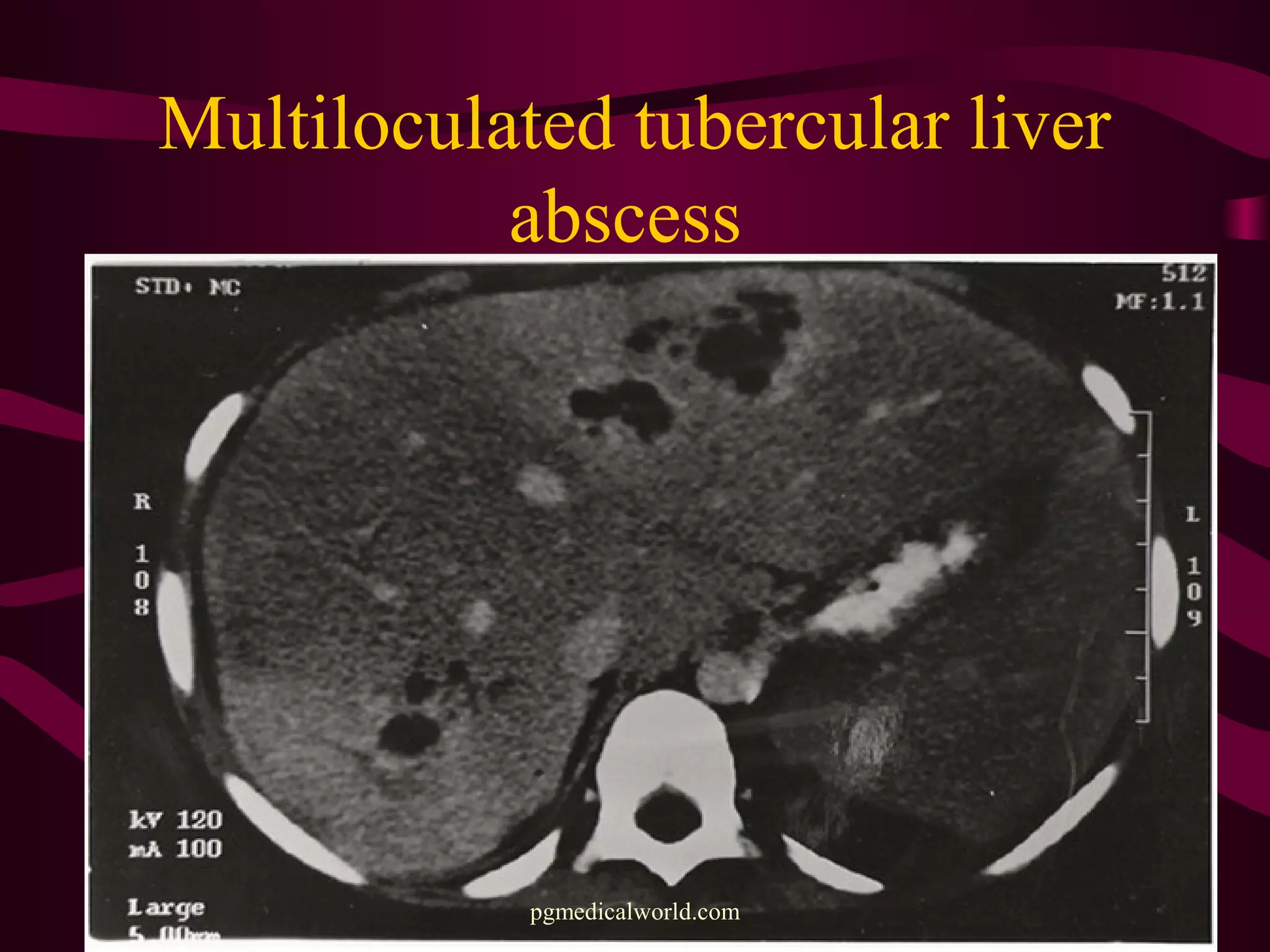
This document provides information on the management of liver abscesses. It discusses the two main types - pyogenic and amebic liver abscesses. For pyogenic liver abscesses, it outlines the etiology, clinical features, investigations, and treatment options including antibiotics, aspiration, percutaneous drainage, and surgical drainage. It also discusses amebic liver abscesses, noting they are more common in tropical areas. It provides details on the pathology, clinical features, diagnosis, and treatment of amebic liver abscesses, which typically involves antibiotics or therapeutic aspiration.